Department of Biostatistics at Epidemiology, Biostatistics and Prevention Institute, University of Zurich, Hirschengraben 84, 8001, Zurich, Switzerland.
Department of Internal Medicine, Horten Centre for Patient Oriented Research and Knowledge Transfer, University of Zurich, Pestalozzistrasse 24, 8032, Zurich, Switzerland.
Sci Rep. 2022 Feb 18;12(1):2821. doi: 10.1038/s41598-022-06797-1.
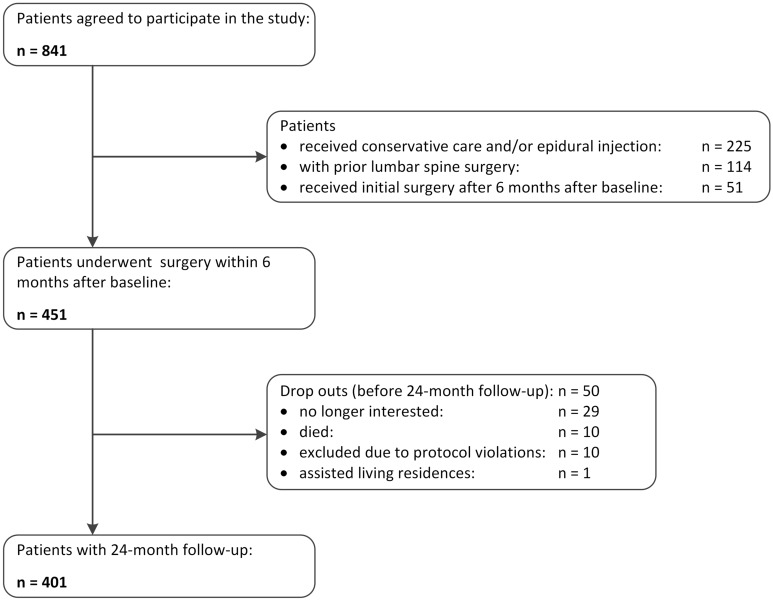
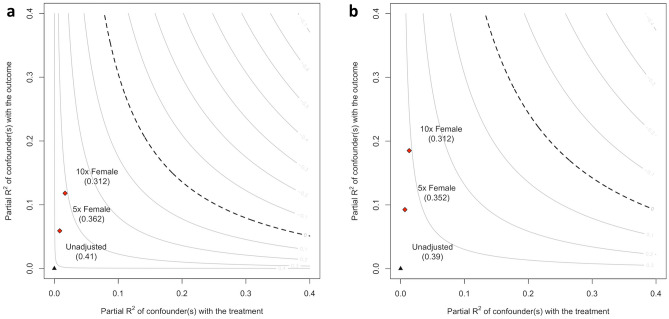
Evidence on the role of depression and anxiety in patients undergoing surgical treatment for symptomatic degenerative lumbar spinal stenosis (DLSS) is conflicting. We aimed to assess the association between depression and anxiety with symptoms and function in patients undergoing surgery for DLSS. Included were patients with symptomatic DLSS participating in a prospective multicentre cohort study who underwent surgery and completed the 24-month follow-up. We used the hospital anxiety and depression scale (HADS) to assess depression/anxiety. We used mixed-effects models to quantify the impact on the primary outcome change in the spinal stenosis measure (SSM) symptoms/function subscale from baseline to 12- and 24-months. Logistic regression analysis was used to quantify the odds of the SSM to reach a minimal clinically important difference (MCID) at 24 months follow-up. The robustness of the results in the presence of unmeasured confounding was quantified using a benchmarking method based on a multiple linear model. Out of 401 patients 72 (17.95%) were depressed and 80 anxious (19.05%). Depression was associated with more symptoms (β = 0.36, 95% confidence interval (CI) 0.20 to 0.51, p < 0.001) and worse function (β = 0.37, 95% CI 0.24 to 0.50, p < 0.001) at 12- and 24-months. Only the association between baseline depression and SSM symptoms/function was robust at 12 and 24 months. There was no evidence for baseline depression/anxiety decreasing odds for a MCID in SSM symptoms and function over time. In patients undergoing surgery for symptomatic DLSS, preoperative depression but not anxiety was associated with more severe symptoms and disability at 12 and 24 months.
手术治疗症状性退行性腰椎管狭窄症(DLSS)患者中抑郁和焦虑作用的证据相互矛盾。我们旨在评估抑郁和焦虑与接受 DLSS 手术患者的症状和功能之间的关联。本研究纳入了参加前瞻性多中心队列研究并接受手术且完成 24 个月随访的症状性 DLSS 患者。我们使用医院焦虑和抑郁量表(HADS)评估抑郁/焦虑。我们使用混合效应模型来量化从基线到 12 个月和 24 个月时脊柱狭窄量表(SSM)症状/功能子量表的主要结局变化的影响。使用逻辑回归分析来量化 SSM 在 24 个月随访时达到最小临床重要差异(MCID)的可能性。使用基于多元线性模型的基准方法来量化存在未测量混杂因素时结果的稳健性。在 401 名患者中,72 名(17.95%)抑郁,80 名(19.05%)焦虑。抑郁与更多的症状(β=0.36,95%置信区间(CI)0.20 至 0.51,p<0.001)和更差的功能(β=0.37,95% CI 0.24 至 0.50,p<0.001)相关,在 12 个月和 24 个月时。只有基线抑郁与 SSM 症状/功能之间的相关性在 12 个月和 24 个月时是稳健的。基线抑郁/焦虑并不能降低 SSM 症状和功能随时间变化的 MCID 的可能性。在接受症状性 DLSS 手术的患者中,术前抑郁但不是焦虑与 12 个月和 24 个月时更严重的症状和残疾相关。