Division of Cardiovascular Surgery, Departments of Surgery and Pediatrics, University of Florida, Gainesville, Florida.
Division of Cardiovascular Surgery, Departments of Surgery and Pediatrics, University of Florida, Gainesville, Florida; Medical Department, SpecialtyCare, Inc, Nashville, Tennessee.
Ann Thorac Surg. 2022 Jul;114(1):61-68. doi: 10.1016/j.athoracsur.2022.01.043. Epub 2022 Feb 18.
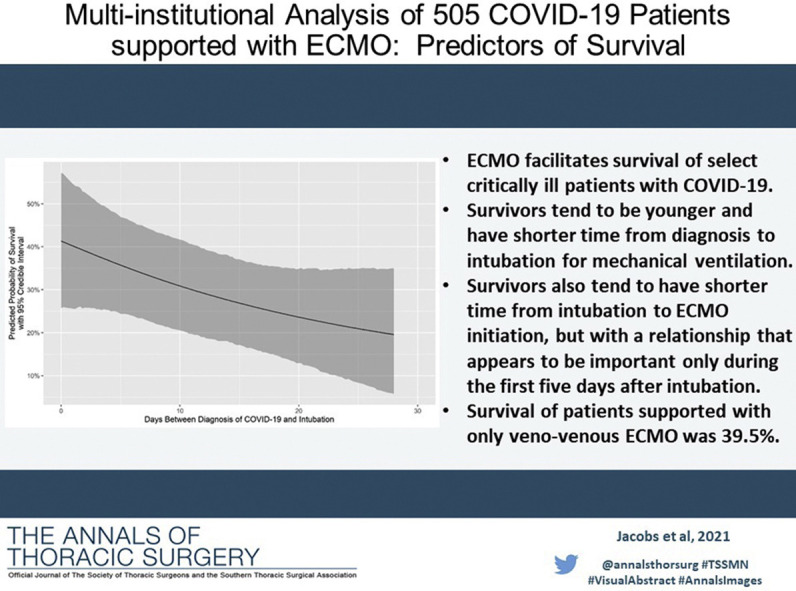
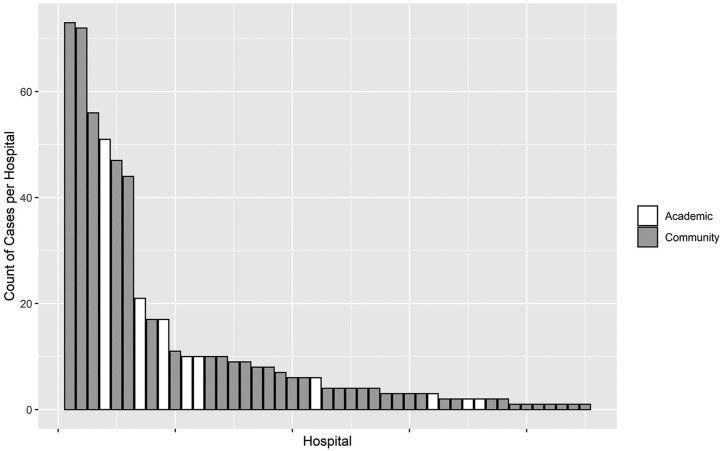
We reviewed our experience with 505 patients with confirmed coronavirus disease-2019 (COVID-19) supported with extracorporeal membrane oxygenation (ECMO) at 45 hospitals and estimated risk factors for mortality.
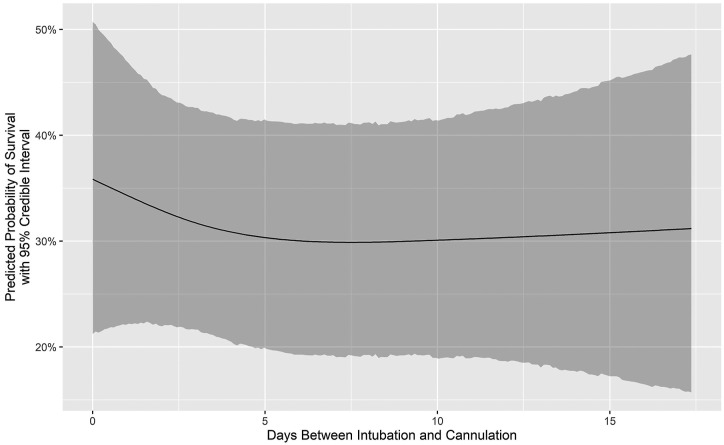
A multi-institutional database was created and used to assess all patients with COVID-19 who were supported with ECMO. A Bayesian mixed-effects logistic regression model was estimated to assess the effect on survival of multiple potential risk factors for mortality, including age at cannulation for ECMO as well as days between diagnosis of COVID-19 and intubation and days between intubation and cannulation for ECMO.
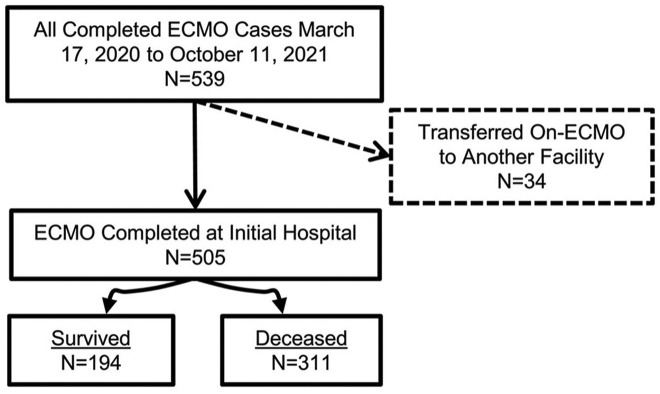
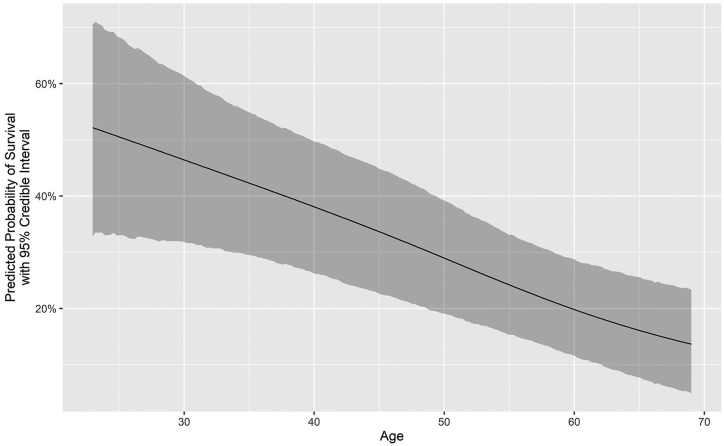
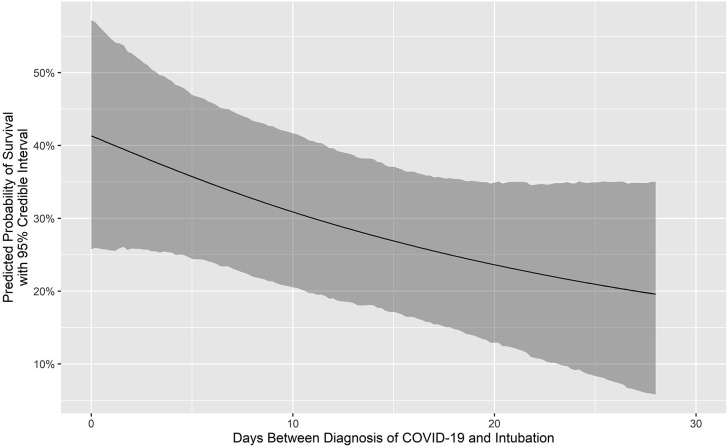
Median time on ECMO was 18 days (interquartile range, 10-29 days). All 505 patients separated from ECMO: 194 patients (38.4%) survived and 311 patients (61.6%) died. Survival with venovenous ECMO was 184 of 466 patients (39.5%), and survival with venoarterial ECMO was 8 of 30 patients (26.7%). Survivors had lower median age (44 vs 51 years, P < .001) and shorter median time interval from diagnosis to intubation (7 vs 11 days, P = .001). Adjusting for several confounding factors, we estimated that an ECMO patient intubated on day 14 after the diagnosis of COVID-19 vs day 4 had a relative odds of survival of 0.65 (95% credible interval, 0.44-0.96; posterior probability of negative effect, 98.5%). Age was also negatively associated with survival: relative to a 38-year-old patient, we estimated that a 57-year-old patient had a relative odds of survival of 0.43 (95% credible interval, 0.30-0.61; posterior probability of negative effect, >99.99%).
ECMO facilitates salvage and survival of select critically ill patients with COVID-19. Survivors tend to be younger and have shorter time from diagnosis to intubation. Survival of patients supported with only venovenous ECMO was 39.5%.
我们回顾了在 45 家医院接受体外膜肺氧合(ECMO)支持的 505 例确诊的 2019 冠状病毒病(COVID-19)患者的经验,并评估了死亡率的相关危险因素。
创建了一个多机构数据库,用于评估所有接受 ECMO 支持的 COVID-19 患者。采用贝叶斯混合效应逻辑回归模型评估了多个可能的死亡率危险因素对生存的影响,包括 ECMO 置管时的年龄以及 COVID-19 诊断与插管之间的天数和插管与 ECMO 置管之间的天数。
ECMO 的中位时间为 18 天(四分位距,10-29 天)。505 例患者全部脱离 ECMO:194 例(38.4%)存活,311 例(61.6%)死亡。静脉-静脉 ECMO 治疗的存活率为 466 例中的 184 例(39.5%),静脉-动脉 ECMO 治疗的存活率为 30 例中的 8 例(26.7%)。存活者的中位年龄较低(44 岁比 51 岁,P<.001),从诊断到插管的中位时间间隔较短(7 天比 11 天,P=.001)。调整了几个混杂因素后,我们估计 COVID-19 诊断后第 14 天与第 4 天插管的 ECMO 患者的生存相对几率为 0.65(95%可信区间,0.44-0.96;负效应的后验概率,98.5%)。年龄也与生存呈负相关:与 38 岁的患者相比,我们估计 57 岁的患者的生存相对几率为 0.43(95%可信区间,0.30-0.61;负效应的后验概率,>99.99%)。
ECMO 有助于抢救和挽救 COVID-19 重症患者。存活者往往更年轻,从诊断到插管的时间更短。仅接受静脉-静脉 ECMO 支持的患者的存活率为 39.5%。