Department of Surgery, Dentistry, Gynecology and Pediatrics, Unit of General and Pancreatic Surgery, University of Verona, Verona, Italy.
Section of Pathology, Department of Pathology and Diagnostics, University of Verona, Verona, Italy.
Ann Surg Oncol. 2022 Jun;29(6):3477-3488. doi: 10.1245/s10434-022-11417-3. Epub 2022 Feb 21.
Implementing a prospective lymphadenectomy protocol, we investigated the nodal yields and metastases per anatomical stations and nodal echelon following upfront pancreatoduodenectomy (PD) for cancer. Next, the relationship between the extension of nodal dissection, the number of examined and positive nodes (ELN/PLN), disease staging and prognosis was assessed.
Lymphadenectomy included stations 5, 6, 8a-p, 12a-b-p, 13, 14a-b, 17, and jejunal mesentery nodes. Data were stratified by N-status, anatomical stations, and nodal echelons. First echelon was defined as stations embedded in the main specimen and second echelon as stations sampled as separate specimens. Recurrence and survival analyses were performed by using standard statistics.
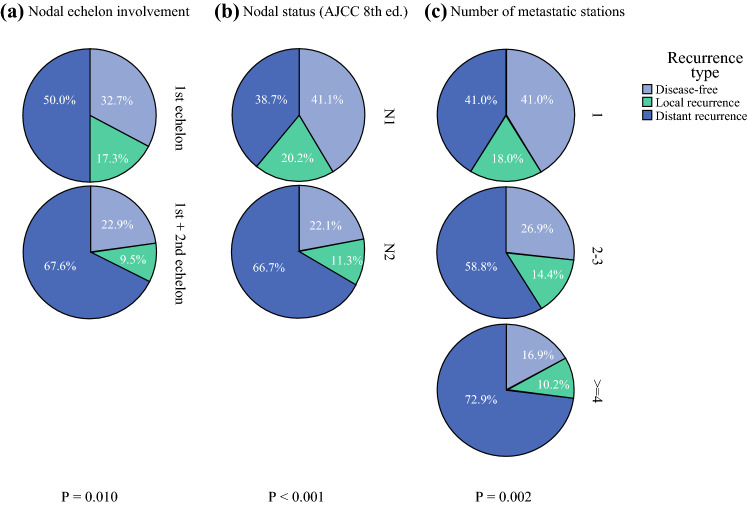
Overall, 424 patients were enrolled from June 2013 through December 2018. The median number of ELN and PLN was 42 (interquartile range [IQR] 34-50) and 4 (IQR 2-8). Node-positive patients were 88.2%. The commonest metastatic sites were stations 13 (77.8%) and 14 (57.5%). The median number of ELN and PLN in the first echelon was 28 (IQR 23-34) and 4 (IQR 1-7). While first-echelon dissection provided enough ELN for optimal nodal staging, the aggregate rate of second-echelon metastases approached 30%. Nodal-related factors associated with recurrence and survival were N-status, multiple metastatic stations, metastases to station 14, and jejunal mesentery nodes.
First-echelon dissection provides adequate number of ELN for optimal staging. Nodal metastases occur mostly at stations 13/14, although second-echelon involvement is frequent. Only station 14 and jejunal mesentery nodes involvement was prognostically relevant. This latter station should be included in the standard nodal map and analyzed pathologically.
我们实施了前瞻性淋巴结清扫方案,研究了癌症患者行胰十二指肠切除术(PD) upfront 时,各解剖站和淋巴结级别的淋巴结检出数和转移数。然后,评估了淋巴结清扫范围、清扫和阳性淋巴结数量(ELN/PLN)、疾病分期和预后之间的关系。
淋巴结清扫包括站 5、6、8a-p、12a-b-p、13、14a-b、17 和空肠系膜淋巴结。数据根据 N 分期、解剖站和淋巴结级分层。第一级定义为嵌入主要标本的站,第二级定义为作为单独标本取样的站。采用标准统计学方法进行复发和生存分析。
2013 年 6 月至 2018 年 12 月共纳入 424 例患者。ELN 和 PLN 的中位数分别为 42(四分位距 [IQR] 34-50)和 4(IQR 2-8)。淋巴结阳性患者占 88.2%。最常见的转移部位是站 13(77.8%)和站 14(57.5%)。第一级淋巴结清扫的 ELN 和 PLN 中位数分别为 28(IQR 23-34)和 4(IQR 1-7)。虽然第一级解剖提供了足够的 ELN 以进行最佳的淋巴结分期,但第二级转移的总发生率接近 30%。与复发和生存相关的淋巴结相关因素包括 N 分期、多个转移站、站 14 转移和空肠系膜淋巴结。
第一级解剖提供了足够数量的 ELN 以进行最佳分期。淋巴结转移主要发生在站 13/14,但第二级受累很常见。只有站 14 和空肠系膜淋巴结受累与预后相关。后者应包括在标准淋巴结图谱中并进行病理分析。