Translational Research in Hepatic Oncology, Liver Unit, IDIBAPS, Hospital Clínic, Universitat de Barcelona, Barcelona, Spain.
Pathology Department & Molecular Biology CORE, Hospital Clinic de Barcelona, Barcelona, Spain.
Gut. 2023 Jan;72(1):129-140. doi: 10.1136/gutjnl-2021-325918. Epub 2022 Feb 23.
We previously reported a characterisation of the hepatocellular carcinoma (HCC) immune contexture and described an immune-specific class. We now aim to further delineate the immunogenomic classification of HCC to incorporate features that explain responses/resistance to immunotherapy.
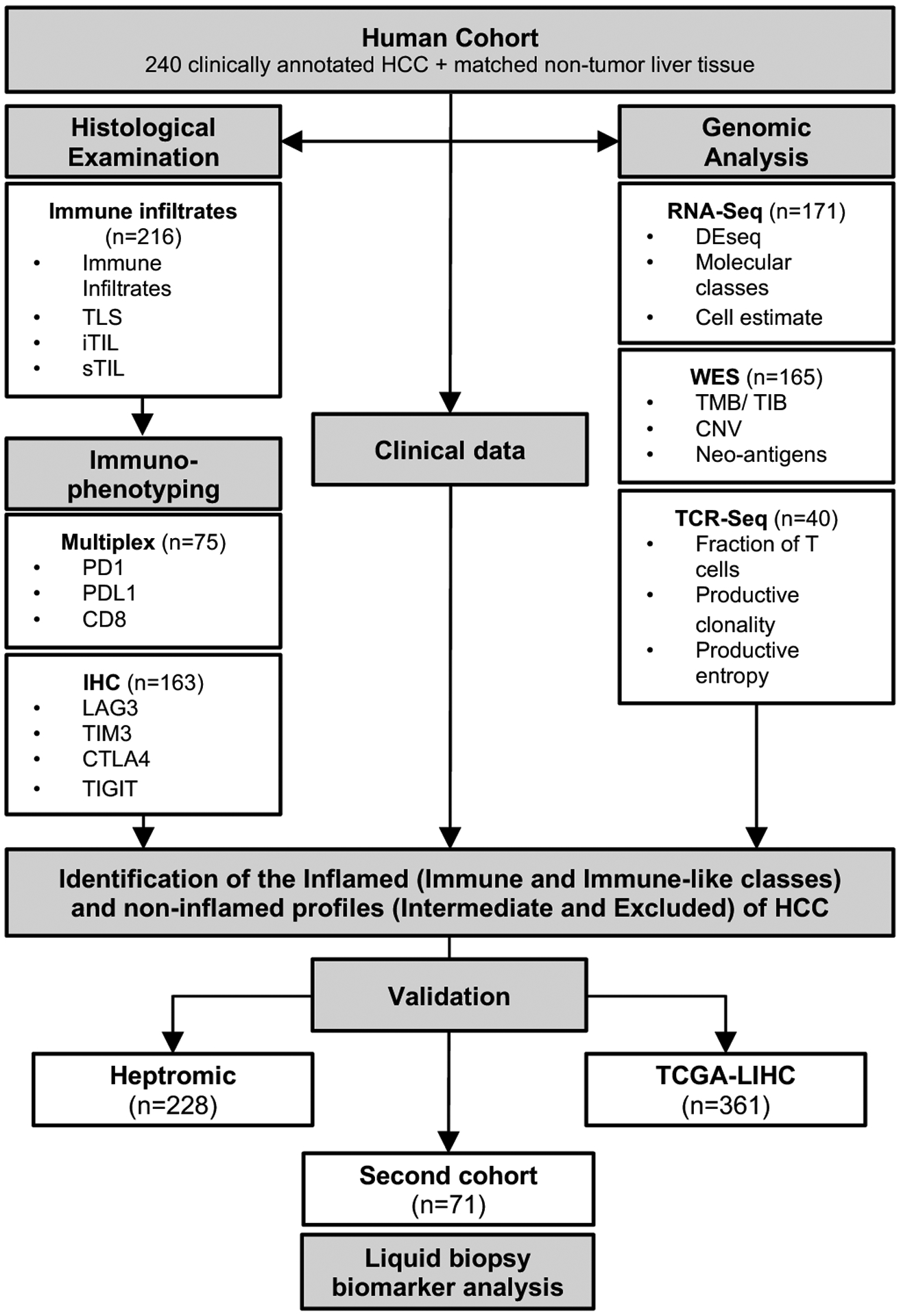
We performed RNA and whole-exome sequencing, T-cell receptor (TCR)-sequencing, multiplex immunofluorescence and immunohistochemistry in a novel cohort of 240 HCC patients and validated our results in other cohorts comprising 660 patients.
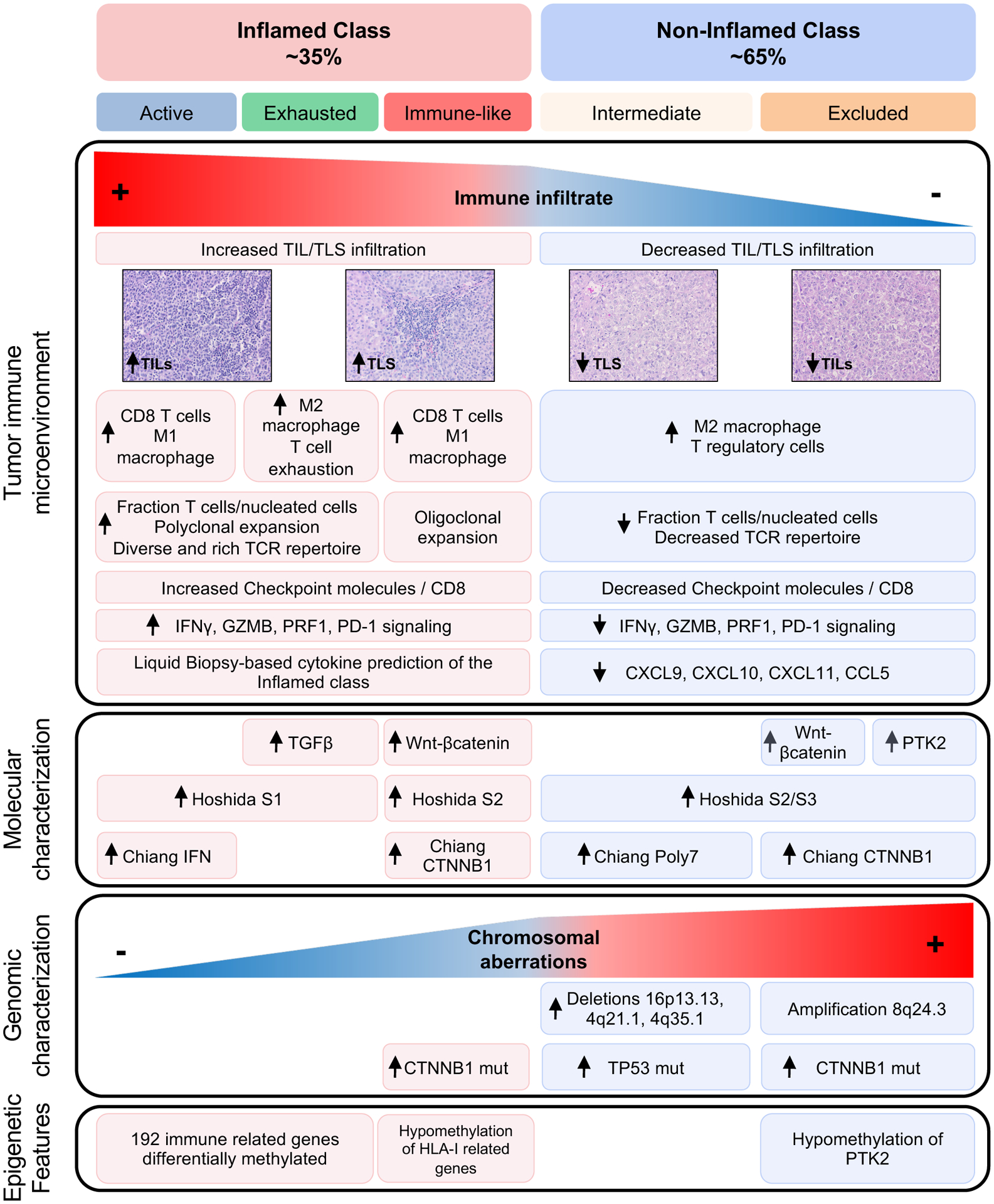
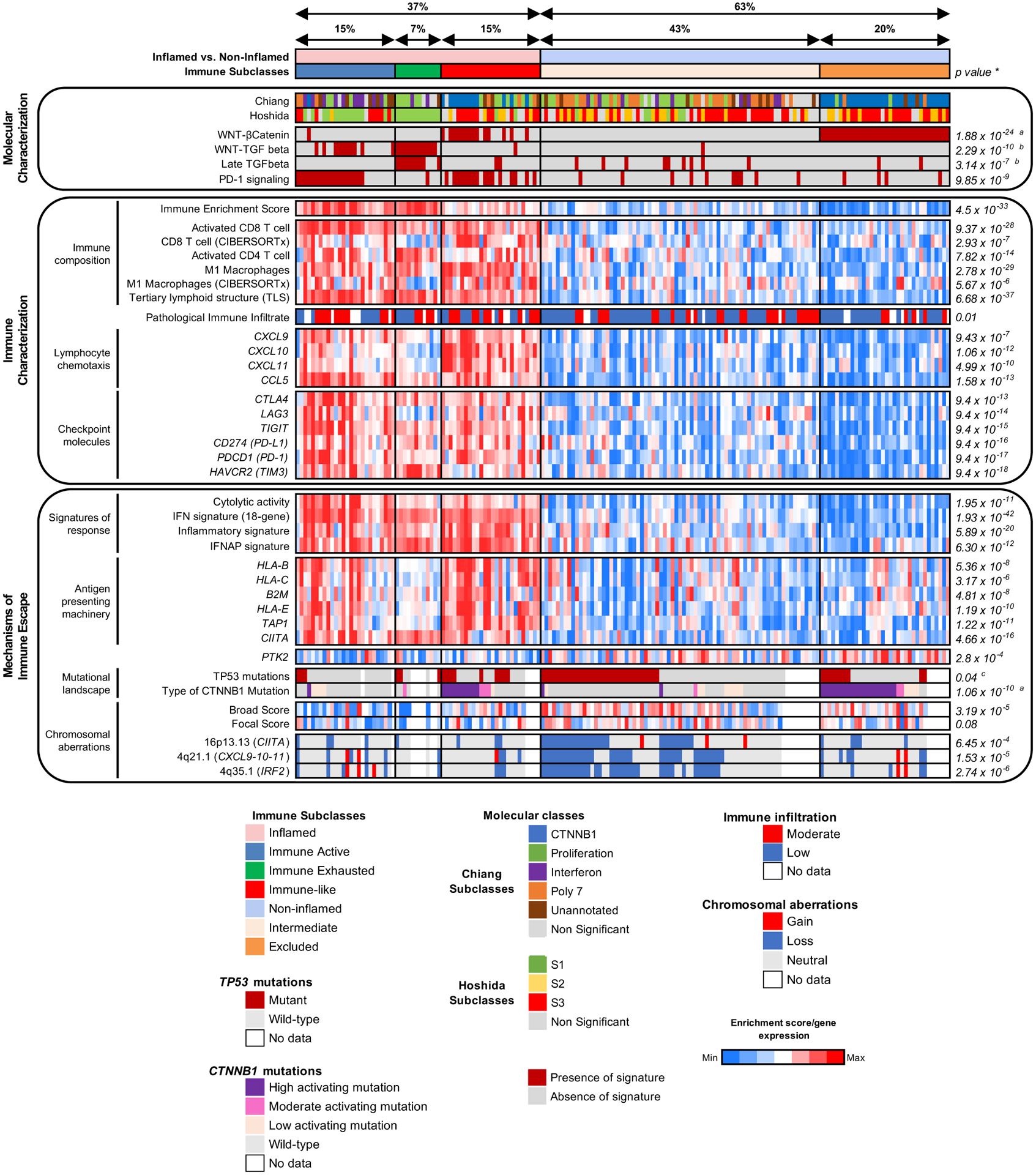
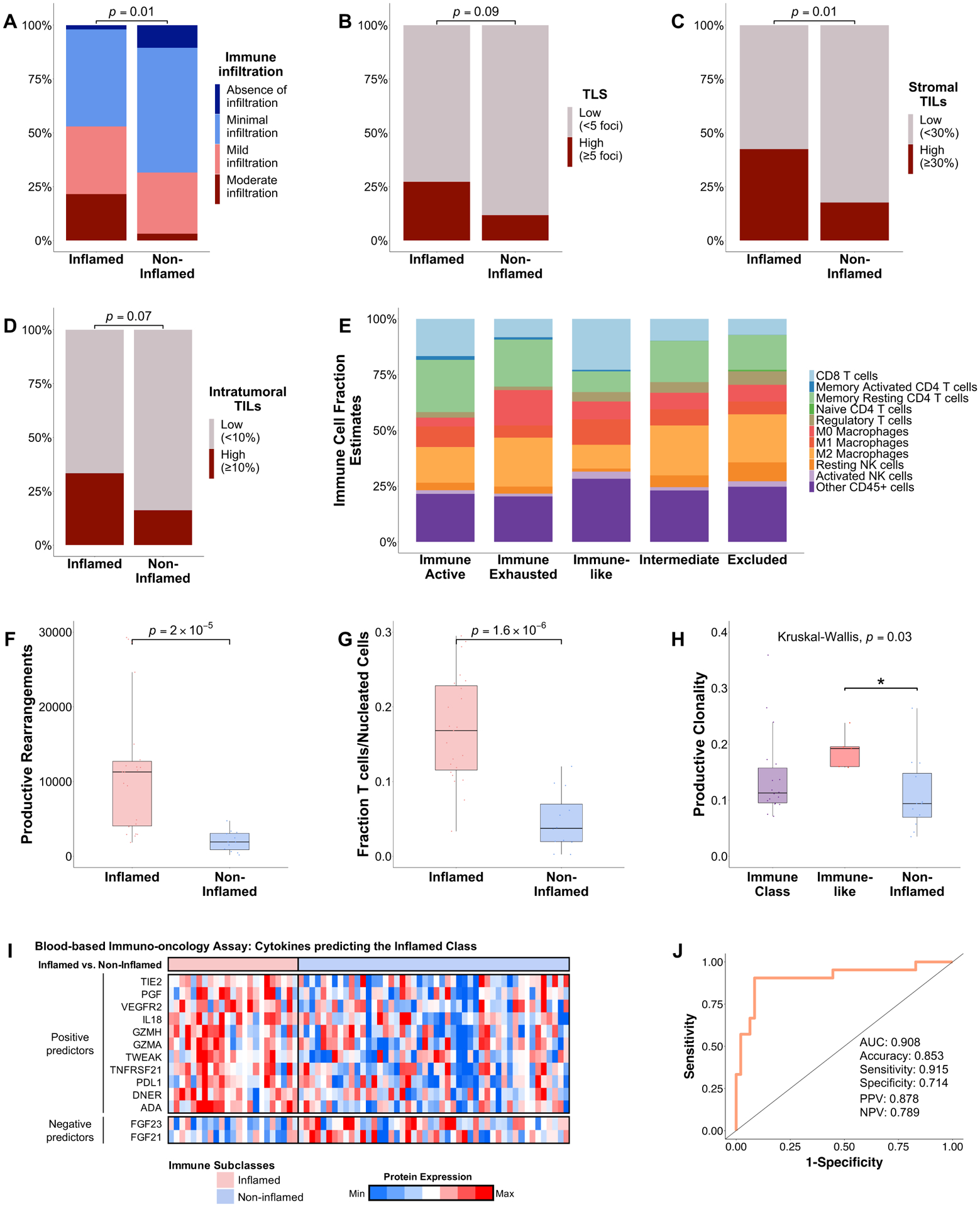
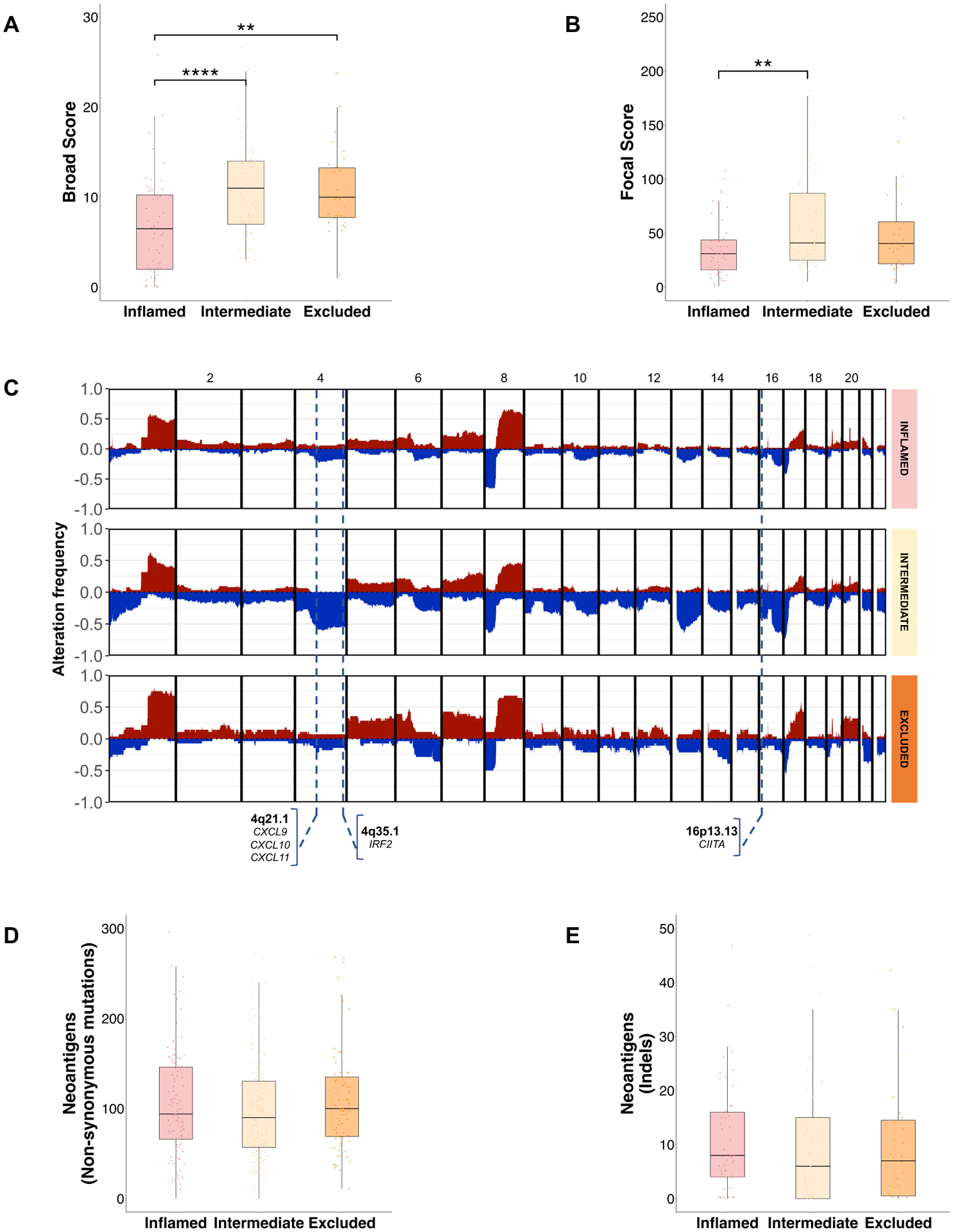
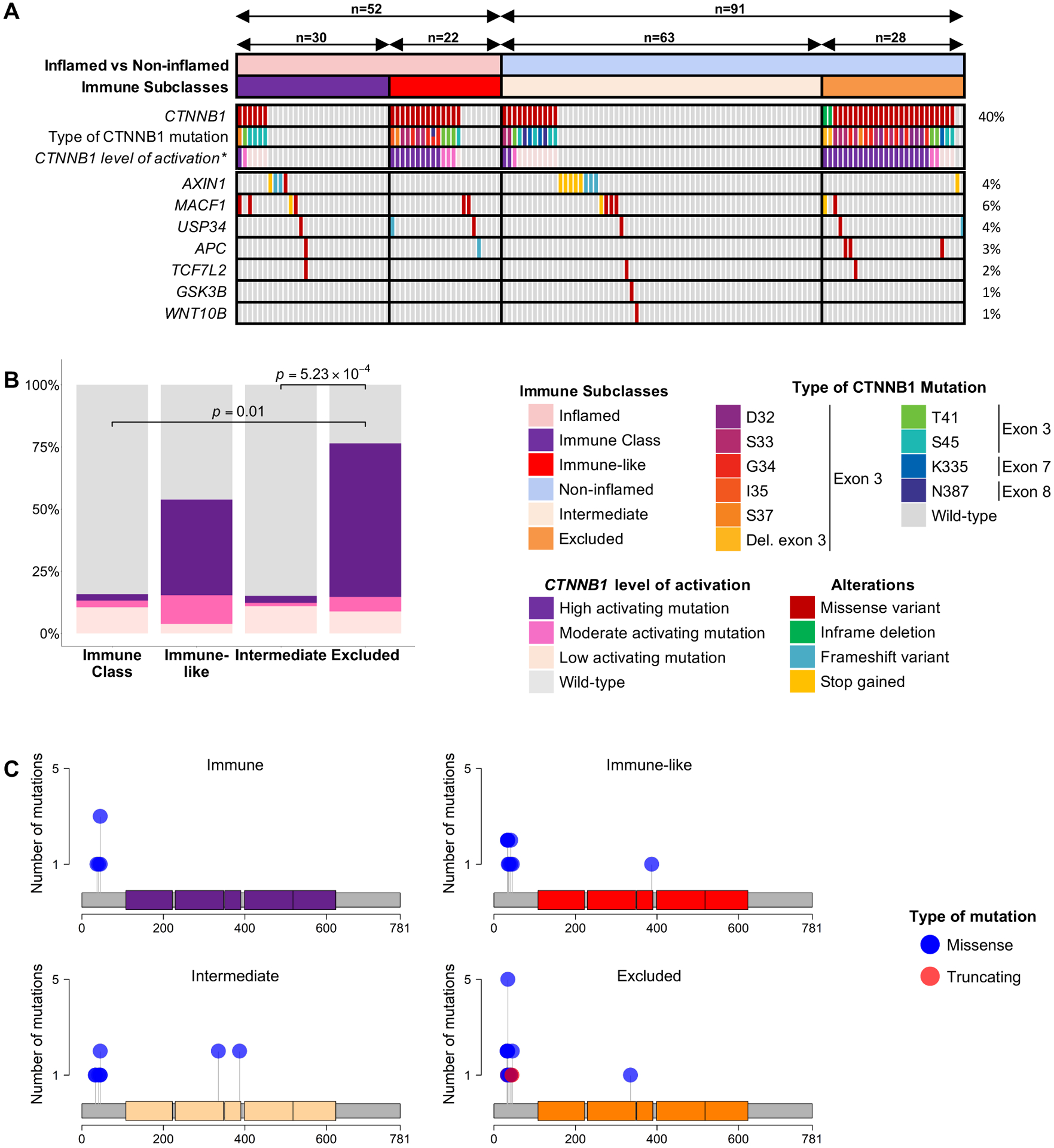
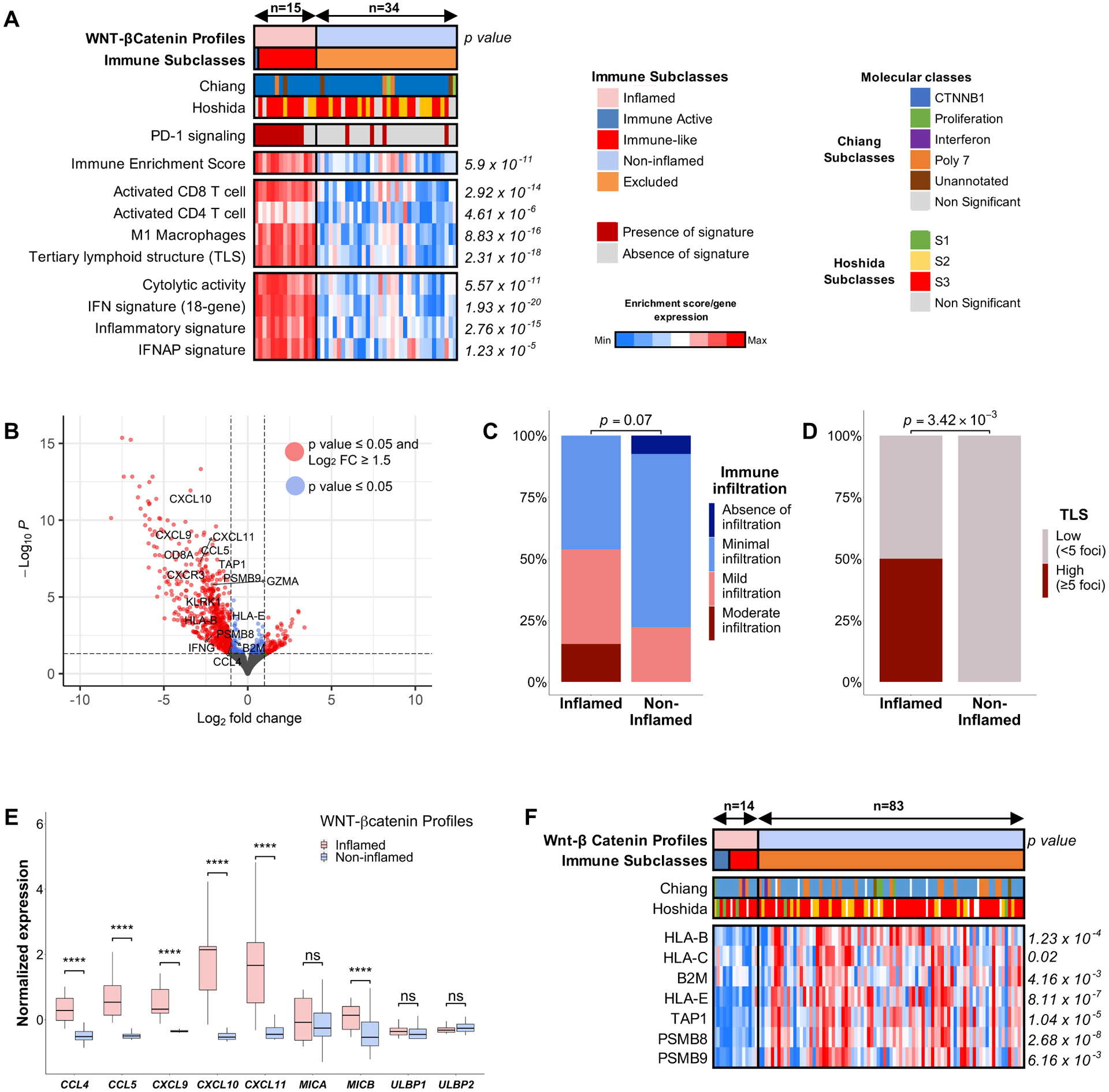
Our integrative analysis led to define: (1) the inflamed class of HCC (37%), which includes the previously reported immune subclass (22%) and a new immune-like subclass (15%) with high interferon signalling, cytolytic activity, expression of immune-effector cytokines and a more diverse T-cell repertoire. A 20-gene signature was able to capture ~90% of these tumours and is associated with response to immunotherapy. Proteins identified in liquid biopsies recapitulated the inflamed class with an area under the ROC curve (AUC) of 0.91; (2) The intermediate class, enriched in mutations (49% vs 29%, p=0.035), and chromosomal losses involving immune-related genes and; (3) the excluded class, enriched in mutations (93% vs 27%, p<0.001) and overexpression due to gene amplification and promoter hypomethylation. mutations outside the excluded class led to weak activation of the Wnt-βcatenin pathway or occurred in HCCs dominated by high interferon signalling and type I antigen presenting genes.
We have characterised the immunogenomic contexture of HCC and defined inflamed and non-inflamed tumours. Two distinct patterns associated with a differential role in immune evasion are described. These features may help predict immune response in HCC.
我们之前对肝细胞癌(HCC)的免疫结构进行了描述,并描述了一个免疫特异的亚型。我们现在的目标是进一步描绘 HCC 的免疫基因组分类,纳入能解释对免疫治疗反应/耐药的特征。
我们对 240 名 HCC 患者进行了 RNA 和全外显子测序、T 细胞受体(TCR)测序、多重免疫荧光和免疫组化分析,并在包含 660 名患者的其他队列中验证了我们的结果。
我们的综合分析导致定义了:(1)HCC 的炎症类(37%),其中包括之前报道的免疫亚类(22%)和一个新的免疫样亚类(15%),具有高干扰素信号、细胞毒性活性、免疫效应细胞因子表达和更多样化的 T 细胞库。一个 20 基因的特征能够捕获约 90%的这些肿瘤,并与免疫治疗的反应相关。在液体活检中鉴定的蛋白质重现了炎症类,其 ROC 曲线下面积(AUC)为 0.91;(2)中间类,富含 突变(49%对 29%,p=0.035),以及涉及免疫相关基因的染色体缺失;(3)排除类,富含 突变(93%对 27%,p<0.001)和由于基因扩增和启动子去甲基化导致的 过表达。排除类之外的 突变导致 Wnt-β-catenin 通路的弱激活,或者发生在干扰素信号和 I 型抗原呈递基因高表达的 HCC 中。
我们已经描述了 HCC 的免疫基因组结构,并定义了炎症和非炎症肿瘤。描述了两种与免疫逃避的不同作用相关的独特 模式。这些特征可能有助于预测 HCC 的免疫反应。