Russu Eliza, Mureşan Adrian Vasile, Kaller Reka, Coşarcă Cătălin Mircea, Arbănaşi Eliza-Mihaela, Arbănaşi Emil-Marian
Clinic of Vascular Surgery, Emergency County Hospital, Târgu-Mureş, Romania.
First Department of Surgery, University of Medicine, Pharmacy, Science and Technology "George Emil Palade", Târgu-Mureş, Romania.
Front Surg. 2022 Feb 7;9:769302. doi: 10.3389/fsurg.2022.769302. eCollection 2022.
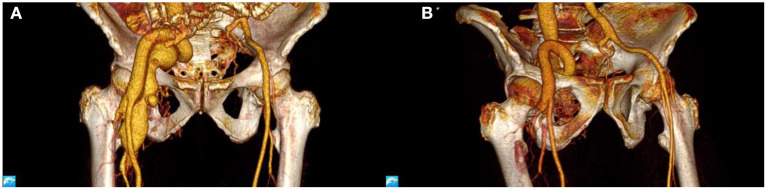
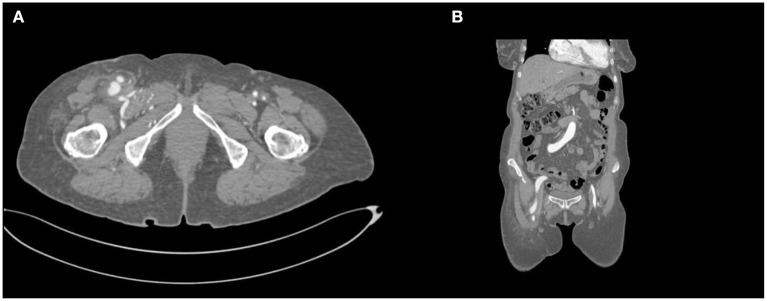
To present the case of a patient with a 9-mm iatrogenic fistula between a branch of the right profunda femoris artery, aneurysmally dilated at ~1.851cm, and the right femoral vein, successfully treated with open surgical ligation.
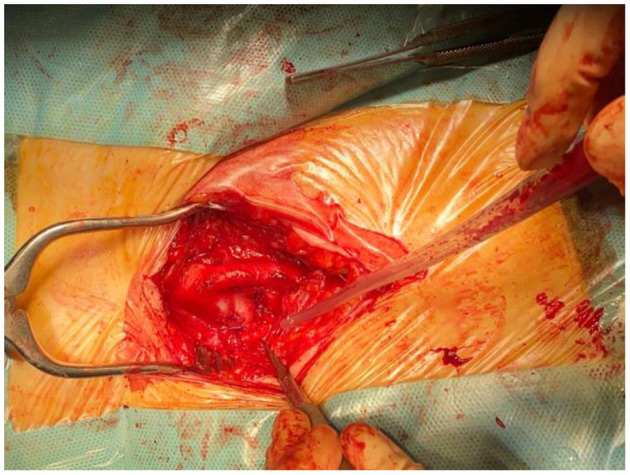
A 70-years-old female was referred to the Vascular Surgery Clinic due to worsening cardiac failure symptoms during the previous year. The medical history included a diagnostic cardiac artery catheterism through a Seldinger technique one year and a half ago. A recent ultrasound described velocities characteristic for a high flow arteriovenous communication in the right groin. Two consecutive cardiology exams, performed at nine months from one another, showed a decrease of almost 21% in the ejection fraction of the left ventricle. An angiography was conducted with the hope of achieving effective percutaneous embolization. Unfortunately, that was not the case. An open repair was scheduled, as the option for a stent-graft deployment was overruled as being too risky, potentially closing several branches of the profunda femoris artery and not fully completing the orifice due to a complicated anatomical positioning. Under local anesthesia, an open ligation was performed in very hostile anatomical conditions. The patient had an uncomplicated evolution and was discharged on the third day, symptom-free.
Iatrogenic arteriovenous fistulas are rare. Clinical presentation diagnoses the case efficiently, vascular imaging being essential for surgical preparation. Though open repair is not the gold standard, there are cases not suitable for the endovascular approach. These patients are eligible for a surgical solution, not without technical challenges.
介绍一例患者,其右股深动脉一分支与右股静脉之间存在一个9毫米的医源性瘘管,该分支动脉瘤样扩张至约1.851厘米,通过开放手术结扎成功治疗。
一名70岁女性因前一年心力衰竭症状加重被转诊至血管外科诊所。病史包括一年半前通过Seldinger技术进行的诊断性心脏动脉导管插入术。最近的超声检查描述了右腹股沟处高流量动静脉交通的特征性血流速度。相隔九个月进行的两次连续心脏检查显示左心室射血分数下降了近21%。进行了血管造影,希望能实现有效的经皮栓塞。不幸的是,情况并非如此。由于支架移植物置入风险太大,可能会封闭股深动脉的几个分支,且由于解剖位置复杂无法完全封闭瘘口,因此排除了这种选择,安排了开放修复手术。在局部麻醉下,在非常不利的解剖条件下进行了开放结扎。患者恢复顺利,第三天无症状出院。
医源性动静脉瘘很少见。临床表现能有效诊断病例,血管成像对手术准备至关重要。虽然开放修复不是金标准,但有些病例不适合血管内治疗方法。这些患者适合手术解决方案,不过存在技术挑战。