Naidoo Kogieleum, Gengiah Santhanalakshmi, Yende-Zuma Nonhlanhla, Mlobeli Regina, Ngozo Jacqueline, Memela Nhlakanipho, Padayatchi Nesri, Barker Pierre, Nunn Andrew, Karim Salim S Abdool
Centre for the AIDS Programme of Research in South Africa (CAPRISA), University of KwaZulu-Natal Nelson R Mandela School of Medicine, Private Bag X7 Congella, Durban 4013, South Africa.
South African Medical Research Council (SAMRC)-CAPRISA-TB-HIV Pathogenesis and Treatment Research Unit, University of KwaZulu-Natal Nelson R Mandela School of Medicine, Durban, South Africa.
EClinicalMedicine. 2022 Feb 12;44:101298. doi: 10.1016/j.eclinm.2022.101298. eCollection 2022 Feb.
HIV-TB treatment integration reduces mortality. Operational implementation of integrated services is challenging. This study assessed the impact of quality improvement (QI) for HIV-TB integration on mortality within primary healthcare (PHC) clinics in South Africa.
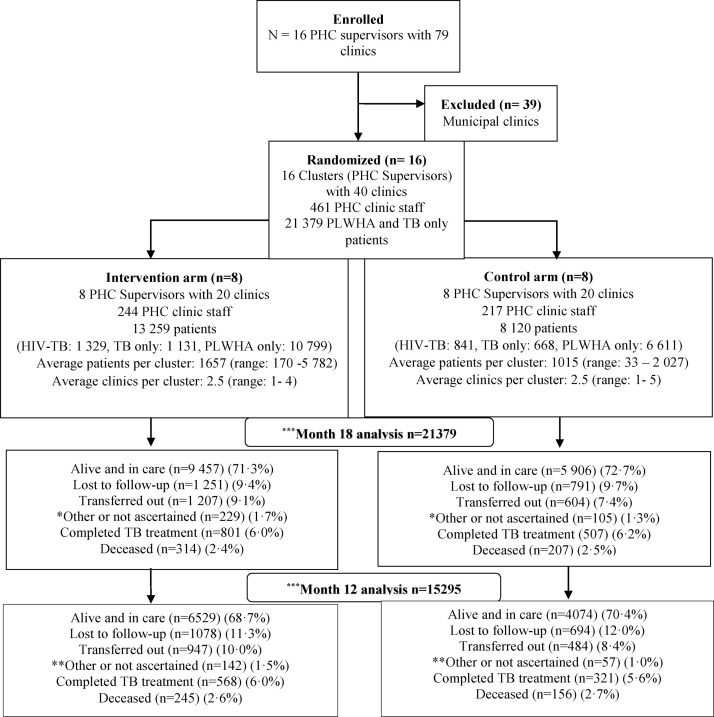
An open-label cluster randomized controlled study was conducted between 2016 and 2018 in 40 rural clinics in South Africa. The study statistician randomized PHC nurse-supervisors 1:1 into 16 clusters (eight nurse-supervisors supporting 20 clinics per arm) to receive QI, supported HIV-TB integration intervention or standard of care (control). Nurse supervisors and clinics under their supervision, based in the study health districts were eligible for inclusion in this study. Nurse supervisors were excluded if their clinics were managed by municipal health (different resource allocation), did not offer co-located antiretroviral therapy (ART) and TB services, services were performed by a single nurse, did not receive non-governmental organisation (NGO) support, patient data was not available for > 50% of attendees. The analysis population consists of all patients newly diagnosed with (i) both TB and HIV (ii) HIV only (among patients previously treated for TB or those who never had TB before) and (iii) TB only (among patients already diagnosed with HIV or those who were never diagnosed with HIV) after QI implementation in the intervention arm, or enrolment in the control arm. Mortality rates was assessed 12 months post enrolment, using unpaired -tests and cox-proportional hazards model. (Clinicaltrials.gov, NCT02654613, registered 01 June 2015, trial closed).
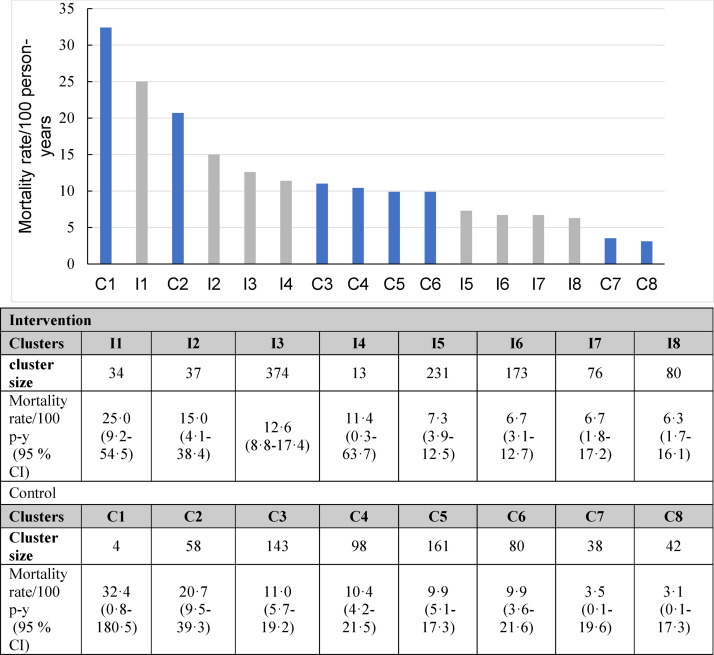
Overall, 21 379 participants were enrolled between December 2016 and December 2018 in intervention and control arm clinics: 1329 and 841 HIV-TB co-infected (10·2%); 10 799 and 6 611 people living with Human Immunodeficiency Virus (HIV)/ acquired immunodeficiency syndrome (AIDS) (PLWHA) only (81·4%); 1 131 and 668 patients with TB only (8·4%), respectively. Average cluster sizes were 1657 (range 170-5782) and 1015 (range 33-2027) in intervention and control arms. By 12 months, 6529 (68·7%) and 4074 (70·4%) were alive and in care, 568 (6·0%) and 321 (5·6%) had completed TB treatment, 1078 (11·3%) and 694 (12·0%) were lost to follow-up, with 245 and 156 deaths occurring in intervention and control arms, respectively. Mortality rates overall [95% confidence interval (CI)] was 4·5 (3·4-5·9) in intervention arm, and 3·8 (2·6-5·4) per 100 person-years in control arm clusters [mortality rate ratio (MRR): 1·19 (95% CI 0·79-1·80)]. Mortality rates among HIV-TB co-infected patients was 10·1 (6·7-15·3) and 9·8 (5·0-18·9) per 100 person-years, [MRR: 1·04 (95% CI 0·51-2·10)], in intervention and control arm clusters, respectively.
HIV-TB integration supported by a QI intervention did not reduce mortality in HIV-TB co-infected patients. Demonstrating mortality benefit from health systems process improvements in real-world operational settings remains challenging. Despite the study being potentially underpowered to demonstrate the effect size, integration interventions were implemented using existing facility staff and infrastructure reflecting the real-world context where most patients in similar settings access care, thereby improving generalizability and scalability of study findings.
Research reported in this publication was supported by South African Medical Research Council (SAMRC), and UK Government's Newton Fund through United Kingdom Medical Research Council (UKMRC).
艾滋病毒与结核病治疗整合可降低死亡率。综合服务的实际实施具有挑战性。本研究评估了南非初级卫生保健(PHC)诊所中艾滋病毒与结核病整合的质量改进(QI)对死亡率的影响。
2016年至2018年期间,在南非的40家农村诊所进行了一项开放标签整群随机对照研究。研究统计人员将初级卫生保健护士监督员按1:1随机分为16个群组(每组8名护士监督员,分别支持20家诊所),以接受质量改进、支持艾滋病毒与结核病整合干预或标准护理(对照)。位于研究卫生区的护士监督员及其监督下的诊所符合纳入本研究的条件。如果诊所由市政卫生部门管理(资源分配不同)、未提供同地抗逆转录病毒治疗(ART)和结核病服务、服务由一名护士提供、未获得非政府组织(NGO)支持、超过50%的就诊者没有患者数据,则排除护士监督员。分析人群包括干预组实施质量改进后或对照组入组后新诊断为(i)结核病和艾滋病毒(ii)仅艾滋病毒(在先前接受过结核病治疗的患者或以前从未患过结核病的患者中)和(iii)仅结核病(在已诊断出艾滋病毒的患者或从未被诊断出艾滋病毒的患者中)的所有患者。在入组12个月后评估死亡率,使用非配对检验和Cox比例风险模型。(Clinicaltrials.gov,NCT02654613,2015年6月1日注册,试验结束)。
总体而言,2016年12月至2018年12月期间,干预组和对照组诊所共纳入21379名参与者:1329名和841名艾滋病毒与结核病合并感染患者(10.2%);仅感染人类免疫缺陷病毒(HIV)/获得性免疫缺陷综合征(AIDS)(PLWHA)的患者分别为10799名和6611名(81.4%);仅患有结核病的患者分别为1131名和668名(8.4%)。干预组和对照组的平均群组规模分别为1657名(范围170 - 5782名)和1015名(范围33 - 2027名)。到12个月时,6529名(68.7%)和4074名(70.4%)存活并接受治疗,568名(6.0%)和3名21(5.6%)完成了结核病治疗,1078名(11.3%)和694名(12.0%)失访,干预组和对照组分别有245例和156例死亡。干预组的总体死亡率[95%置信区间(CI)]为每100人年4.5(3.4 - 5.9),对照组群组为每100人年3.8(2.6 - 5.4)[死亡率比(MRR):1.19(95% CI 0.79 - 1.80)]。艾滋病毒与结核病合并感染患者的死亡率在干预组和对照组群组中分别为每100人年10.1(6.7 - 15.3)和9.8(5.0 - 18.9),[MRR:1.04(95% CI 0.51 - 2.10)]。
由质量改进干预支持的艾滋病毒与结核病整合并未降低艾滋病毒与结核病合并感染患者的死亡率。在实际操作环境中证明卫生系统流程改进对死亡率的益处仍然具有挑战性。尽管该研究可能没有足够的效力来证明效应大小,但整合干预是利用现有设施工作人员和基础设施实施的,反映了大多数类似环境中的患者获得护理的实际情况,从而提高了研究结果的普遍性和可扩展性。
本出版物中报告的研究得到了南非医学研究理事会(SAMRC)以及英国政府牛顿基金通过英国医学研究理事会(UKMRC)的支持。