Munkácsy Gyöngyi, Santarpia Libero, Győrffy Balázs
TTK Cancer Biomarker Research Group, Institute of Enzymology, Magyar Tudósok Körútja 2, 1117 Budapest, Hungary.
2nd Department of Pediatrics, Semmelweis University, Tűzoltó Utca 7-9, 1094 Budapest, Hungary.
Biomedicines. 2022 Jan 24;10(2):248. doi: 10.3390/biomedicines10020248.
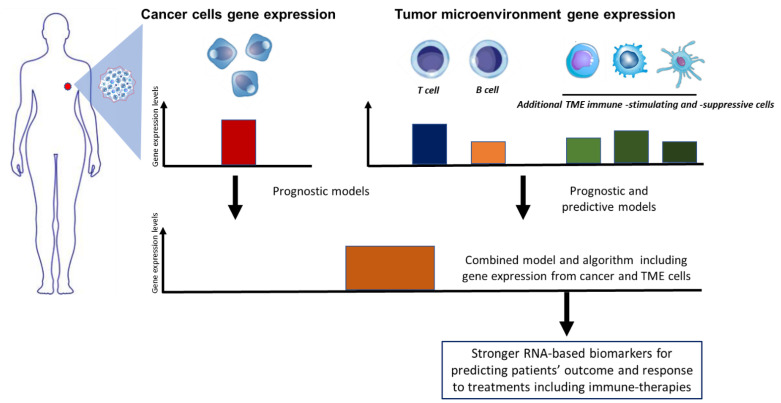
Patients with early-stage hormone receptor-positive, human epidermal growth factor receptor 2-negative (HER2-) breast cancer (BC) are typically treated with surgery, followed by adjuvant systemic endocrine therapy with or without adjuvant chemotherapy and radiation therapy. Current guidelines regarding the use of adjuvant systemic therapy depend on clinical and pathological factors, such as the morphological assessment of tumor subtype; histological grade; tumor size; lymphovascular invasion; and lymph node status combined with estrogen receptor, progesterone receptor, and HER2 biomarker profiles assessed using immunohistochemistry and in situ hybridization. Additionally, the prognostic and predictive value of tumor-infiltrating lymphocytes and their composition is emerging as a key marker in triple negative (TNBC) and HER2-enriched molecular breast tumor subtypes. However, all these factors do not necessarily reflect the molecular heterogeneity and complexity of breast cancer. In the last two decades, gene expression signatures or profiling (GEP) tests have been developed to predict the risk of disease recurrence and estimate the potential benefit of receiving adjuvant systemic chemotherapy in patients with luminal breast cancer. GEPs have been utilized to help physicians to refine decision-making process, complementing clinicopathological parameters, and can now be used to classify the risk of recurrence and tailoring personalized treatments. Several clinical trials using GEPs validate the increasing value of such assays in different clinical settings, addressing relevant clinical endpoints. Finally, the recent approval of immune checkpoint inhibitors in TNBC and the increasing use of immunotherapy in different molecular BC populations highlight the opportunity to refine current GEPs by including a variety of immune-related genes that may help to improve predicting drug response and finetune prognosis.
早期激素受体阳性、人表皮生长因子受体2阴性(HER2-)乳腺癌(BC)患者通常先接受手术治疗,随后根据情况接受辅助全身内分泌治疗,可联合或不联合辅助化疗及放疗。目前关于辅助全身治疗使用的指南取决于临床和病理因素,如肿瘤亚型的形态学评估;组织学分级;肿瘤大小;淋巴管浸润;以及结合使用免疫组织化学和原位杂交评估的雌激素受体、孕激素受体和HER2生物标志物谱的淋巴结状态。此外,肿瘤浸润淋巴细胞及其组成的预后和预测价值正在成为三阴性(TNBC)和HER2富集分子型乳腺肿瘤亚型的关键标志物。然而,所有这些因素并不一定能反映乳腺癌的分子异质性和复杂性。在过去二十年中,已经开发了基因表达特征或谱分析(GEP)测试,以预测管腔型乳腺癌患者疾病复发的风险,并估计接受辅助全身化疗的潜在益处。GEP已被用于帮助医生完善决策过程,补充临床病理参数,现在可用于对复发风险进行分类并制定个性化治疗方案。多项使用GEP的临床试验证实了此类检测在不同临床环境中的价值不断增加,涉及相关临床终点。最后,免疫检查点抑制剂最近在TNBC中的获批以及免疫疗法在不同分子型BC人群中的使用增加,凸显了通过纳入各种可能有助于改善药物反应预测和微调预后的免疫相关基因来完善当前GEP的机会。