Butt Batool, Hussain Tajamul, Jarrar Mu'taman, Khalid Kashaf, Albaker Waleed, Ambreen Asma, Waheed Yasir
Department of Medicine, Foundation University Islamabad, Islamabad 44000, Pakistan.
Research Chair for Biomedical Application of Nanomaterials, Biochemistry Department, College of Science, King Saud University, Riyadh 11451, Saudi Arabia.
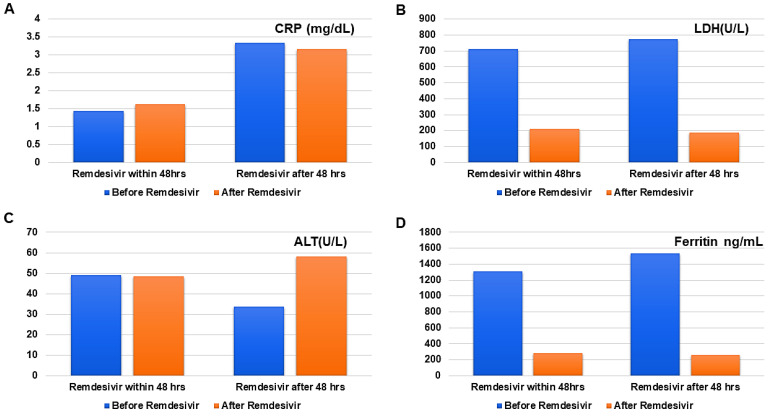
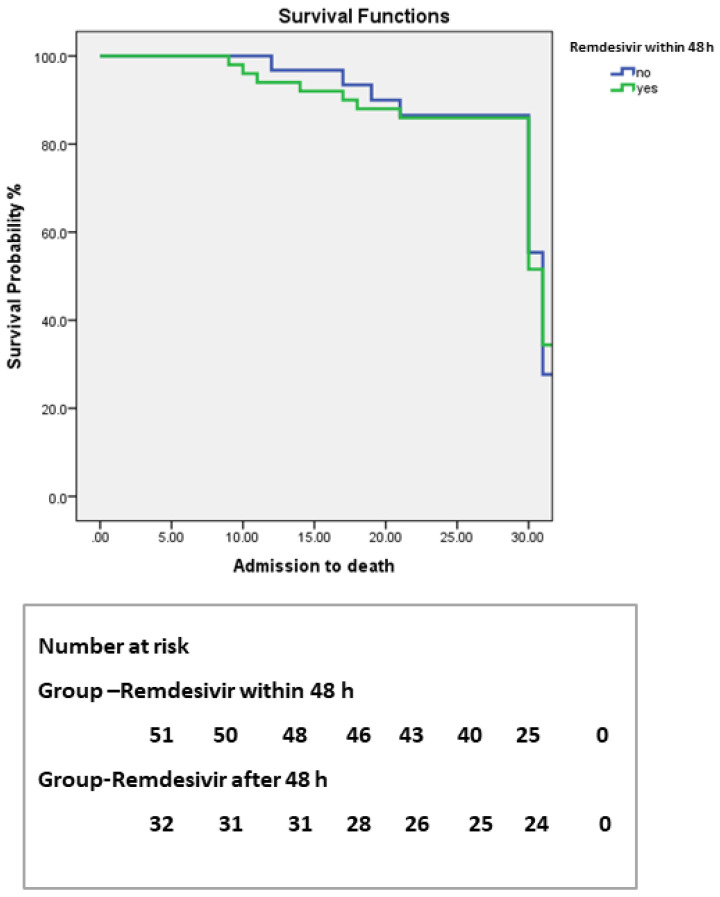
Antibiotics (Basel). 2022 Jan 25;11(2):156. doi: 10.3390/antibiotics11020156.
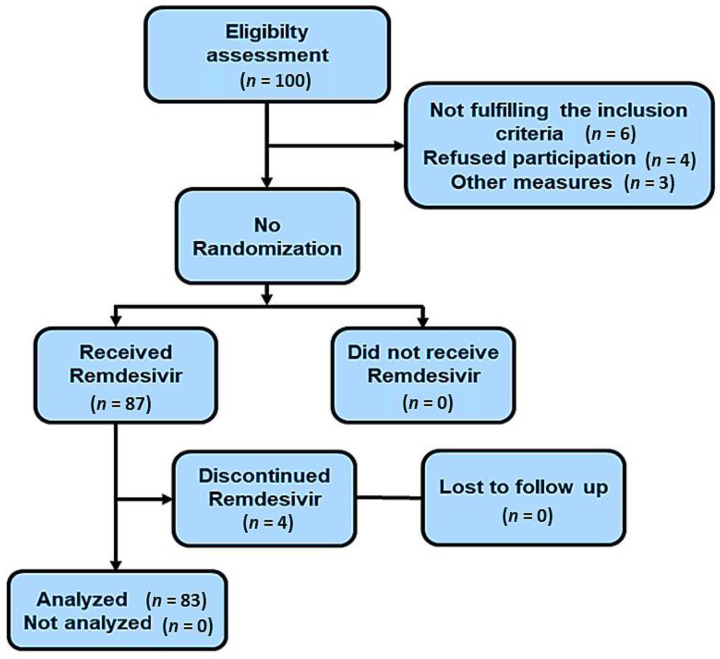
(1) Background: Immune compromised hemodialysis patients are more likely to develop COVID-19 infections, which increase the risk of mortality. The benefits of Remdesivir, despite less literature support on its effectiveness in dialysis patients due to renal toxicity, can outweigh the risks if prescribed early. The aim of this study was to evaluate the efficacy of Remdesivir on the 30-day in-hospital clinical outcome of hemodialysis population with COVID-19 infection and safety endpoints of adverse events. (2) Study design: A prospective quasi-experimental study design was used in the study. (3) Methods: The sample population consisted of 83 dialysis patients with COVID-19 who were administered Remdesivir at a dose of 100 mg before hemodialysis, as per hospital protocol. After the treatment with Remdesivir, we assessed the outcomes across two endpoints, namely primary (surviving vs. dying) as well as clinical and biochemical changes (ferritin, liver function test, C-reactive protein, oxygen requirements, and lactate dehydrogenase levels) and secondary (adverse effects, such as diarrhea, rise in ALT). In Kaplan-Meier analysis, the survival probabilities were compared between patients who received Remdesivir within 48 h of diagnosis and those who received it after 48 h. Cox regression analysis was employed to determine the predictors of outcome. (4) Results: Of the 83 patients, 91.5% survived and 8.4% died. Remdesivir administration did not reduce the death rate overall. Hospital stays were shorter ( = 0.03) and a nasopharyngeal swab for COVID-19 was negative earlier ( = 0.001) in survivors who had received Remdesivir within 48 h of diagnosis compared to those who had received Remdesivir after 48 h. The only variables linked to the 30-day mortality were serum CRP ( = 0.028) and TLC ( = 0.013). No major adverse consequences were observed with Remdesivir. (5) Conclusions: Remdesivir has the potential to shorten the recovery time for dialysis patients if taken within 48 h of onset of symptoms, without any adverse effects.
(1) 背景:免疫功能低下的血液透析患者更易感染新冠病毒,这增加了死亡风险。尽管关于瑞德西韦对透析患者有效性的文献支持较少,因其存在肾毒性,但早期给药时其益处可能超过风险。本研究的目的是评估瑞德西韦对新冠病毒感染的血液透析人群30天院内临床结局及不良事件安全终点的疗效。(2) 研究设计:本研究采用前瞻性准实验研究设计。(3) 方法:样本人群包括83例新冠病毒感染的透析患者,按照医院方案,在血液透析前给予100mg瑞德西韦。在使用瑞德西韦治疗后,我们评估了两个终点的结局,即主要终点(存活与死亡)以及临床和生化变化(铁蛋白、肝功能检查、C反应蛋白、氧需求和乳酸脱氢酶水平)和次要终点(不良反应,如腹泻、谷丙转氨酶升高)。在Kaplan-Meier分析中,比较了在诊断后48小时内接受瑞德西韦治疗的患者和48小时后接受治疗的患者的生存概率。采用Cox回归分析确定结局的预测因素。(4) 结果:83例患者中,91.5%存活,8.4%死亡。总体而言,瑞德西韦给药并未降低死亡率。与诊断后48小时后接受瑞德西韦治疗的幸存者相比,诊断后48小时内接受瑞德西韦治疗的幸存者住院时间更短(P = 0.03),新冠病毒鼻咽拭子转阴更早(P = 0.001)。与30天死亡率相关的唯一变量是血清C反应蛋白(P = 0.028)和白细胞计数(P = 0.013)。未观察到瑞德西韦有重大不良后果。(5) 结论:如果在症状出现后48小时内服用,瑞德西韦有可能缩短透析患者的恢复时间,且无任何不良反应。