Biostatistics Research Branch, National Institute of Allergy and Infectious Diseases, Rockville, Maryland, USA.
Clinical Monitoring Research Program Directorate, Frederick National Laboratory for Cancer Research, Frederick, Maryland, USA.
Clin Infect Dis. 2022 Jul 6;74(12):2209-2217. doi: 10.1093/cid/ciab712.
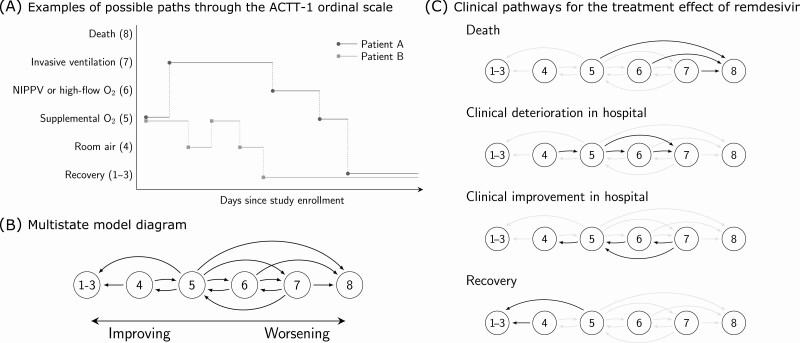
The Adaptive Coronavirus Disease 2019 (COVID-19) Treatment Trial-1 (ACTT-1) found that remdesivir therapy hastened recovery in patients hospitalized with COVID-19, but the pathway for this improvement was not explored. We investigated how the dynamics of clinical progression changed along 4 pathways: recovery, improvement in respiratory therapy requirement, deterioration in respiratory therapy requirement, and death.
We analyzed trajectories of daily ordinal severity scores reflecting oxygen requirements of 1051 patients hospitalized with COVID-19 who participated in ACTT-1. We developed competing risks models that estimate the effect of remdesivir therapy on cumulative incidence of clinical improvement and deterioration, and multistate models that utilize the entirety of each patient's clinical course to characterize the effect of remdesivir on progression along the 4 pathways above.
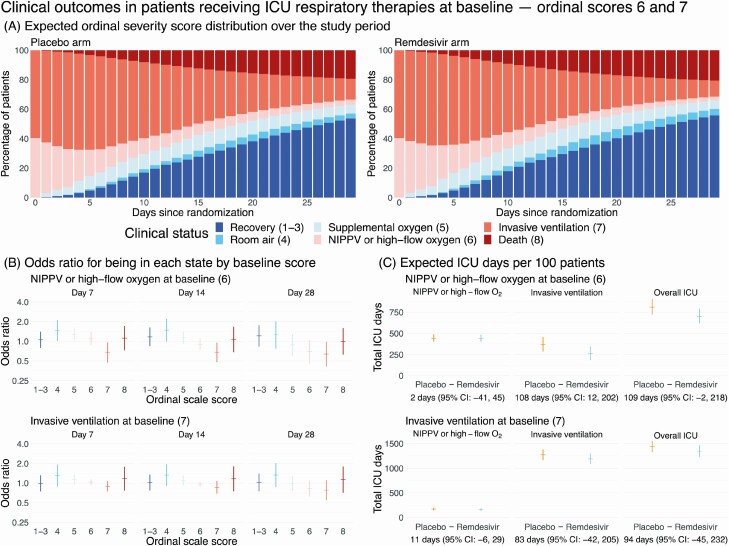
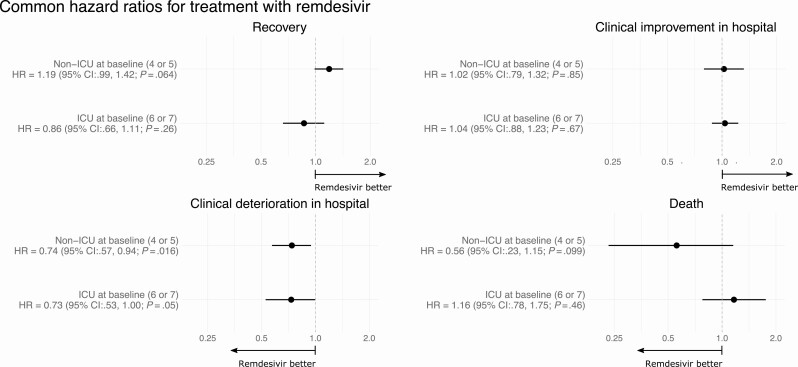
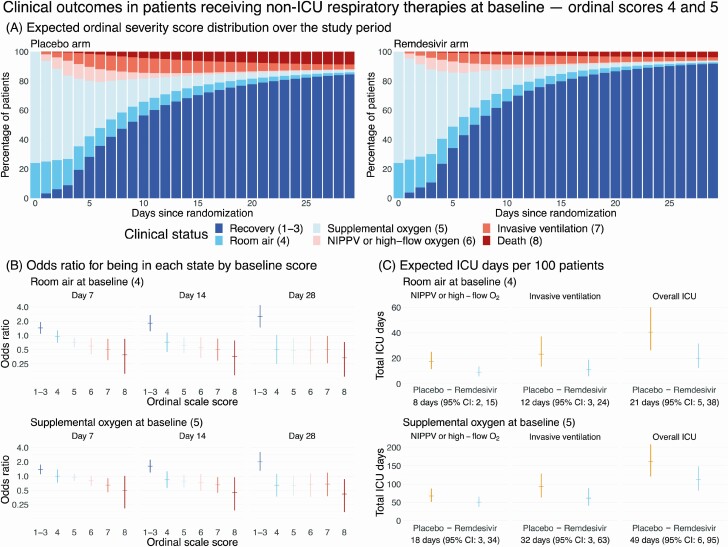
Based on a competing risks analysis, remdesivir reduced clinical deterioration (hazard ratio [HR], 0.73; 95% confidence interval [CI]: .59-.91) and increased clinical improvement (HR, 1.22; 95% CI: 1.08, 1.39) relative to baseline. Our multistate models indicate that remdesivir inhibits worsening to ordinal scores of greater clinical severity among patients on room air or low-flow oxygen (HR, 0.74; 95% CI: .57-.94) and among patients receiving mechanical ventilation or high-flow oxygen/noninvasive positive-pressure ventilation (HR, 0.73; 95% CI: .53-1.00) at baseline. We also find that remdesivir reduces expected intensive care respiratory therapy utilization among patients not mechanically ventilated at baseline.
Remdesivir speeds time to recovery by preventing worsening to clinical states that would extend the course of hospitalization and increase intensive respiratory support, thereby reducing the overall demand for hospital care.
适应性 2019 年冠状病毒病(COVID-19)治疗试验-1(ACTT-1)发现,瑞德西韦治疗可加快 COVID-19 住院患者的康复,但未探索改善的途径。我们研究了临床进展的动态如何通过以下 4 种途径发生变化:康复、呼吸治疗需求改善、呼吸治疗需求恶化和死亡。
我们分析了 1051 名参加 ACTT-1 的 COVID-19 住院患者的每日等级严重程度评分的变化轨迹,这些评分反映了对氧气的需求。我们开发了竞争风险模型,该模型估计瑞德西韦治疗对临床改善和恶化的累积发生率的影响,以及多状态模型,该模型利用每位患者的临床过程的全部内容来描述瑞德西韦对上述 4 种途径的进展的影响。
基于竞争风险分析,瑞德西韦降低了临床恶化的风险(危险比[HR],0.73;95%置信区间[CI]:0.59-0.91)并增加了临床改善的风险(HR,1.22;95%CI:1.08,1.39)与基线相比。我们的多状态模型表明,瑞德西韦抑制了在基线时接受空气或低流量氧气治疗的患者(HR,0.74;95%CI:0.57-0.94)和接受机械通气或高流量氧气/无创正压通气治疗的患者(HR,0.73;95%CI:0.53-1.00)向更严重临床严重程度等级的恶化。我们还发现,瑞德西韦降低了基线时未接受机械通气的患者对重症监护呼吸治疗的预期利用率。
瑞德西韦通过防止向可能延长住院时间和增加强化呼吸支持的临床状态恶化,从而缩短整体住院需求,加快恢复速度。