Mena-Vázquez Natalia, Redondo-Rodríguez Rocío, Rojas-Gimenez Marta, Romero-Barco Carmen María, Manrique-Arija Sara, Ortega-Castro Rafaela, Hidalgo Conde Ana, Arnedo Díez de Los Ríos Rocío, Cabrera César Eva, Espildora Francisco, Aguilar-Hurtado María Carmen, Añón-Oñate Isabel, Pérez-Albaladejo Lorena, Abarca-Costalago Manuel, Ureña-Garnica Inmaculada, Velloso-Feijoo Maria Luisa, Irigoyen-Oyarzábal Maria Victoria, Fernández-Nebro Antonio
Instituto de Investigación Biomédica de Málaga (IBIMA), 29010 Málaga, Spain.
UGC de Reumatología, Hospital Regional Universitario de Málaga, 29009 Málaga, Spain.
J Clin Med. 2022 Feb 10;11(4):927. doi: 10.3390/jcm11040927.
To analyze the efficacy and safety of rituximab (RTX) in connective tissue disease associated with interstitial lung disease (CTD-ILD).
We performed a multicenter, prospective, observational study of patients with CTD-ILD receiving rituximab between 2015 and 2020. The patients were assessed using high-resolution computed tomography and pulmonary function tests at baseline, at 12 months, and at the end of follow-up. The main outcome measure at the end of follow-up was forced vital capacity (FVC) > 10% or diffusing capacity of the lungs for carbon monoxide (DLCO) > 15% and radiological progression or death. We recorded clinical characteristics, time to initiation of RTX, concomitant treatment, infections, and hospitalization. A Cox regression analysis was performed to identify factors associated with worsening ILD.
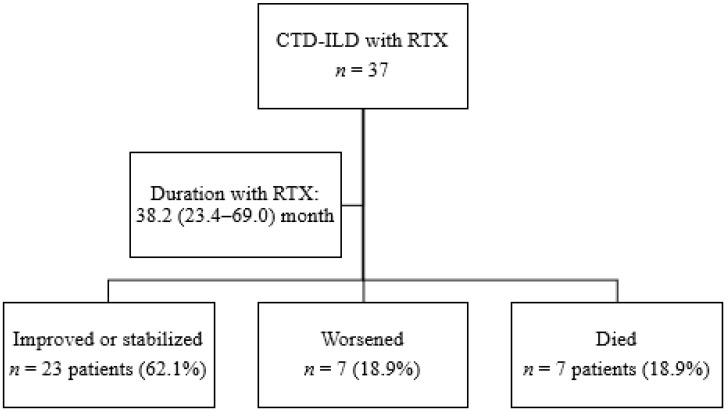
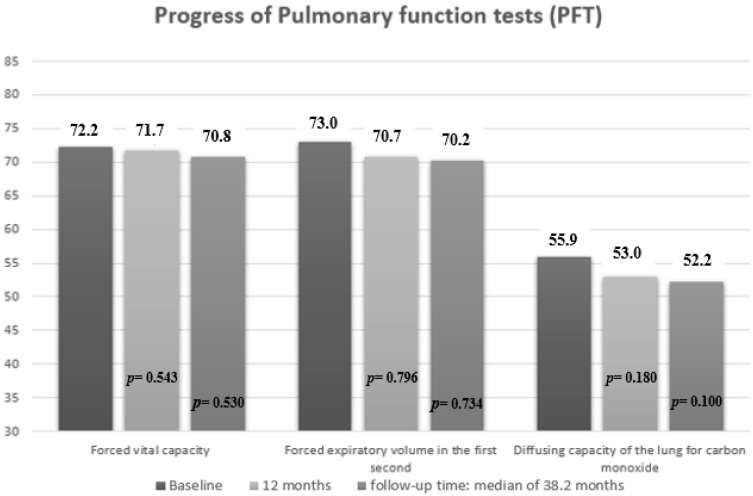
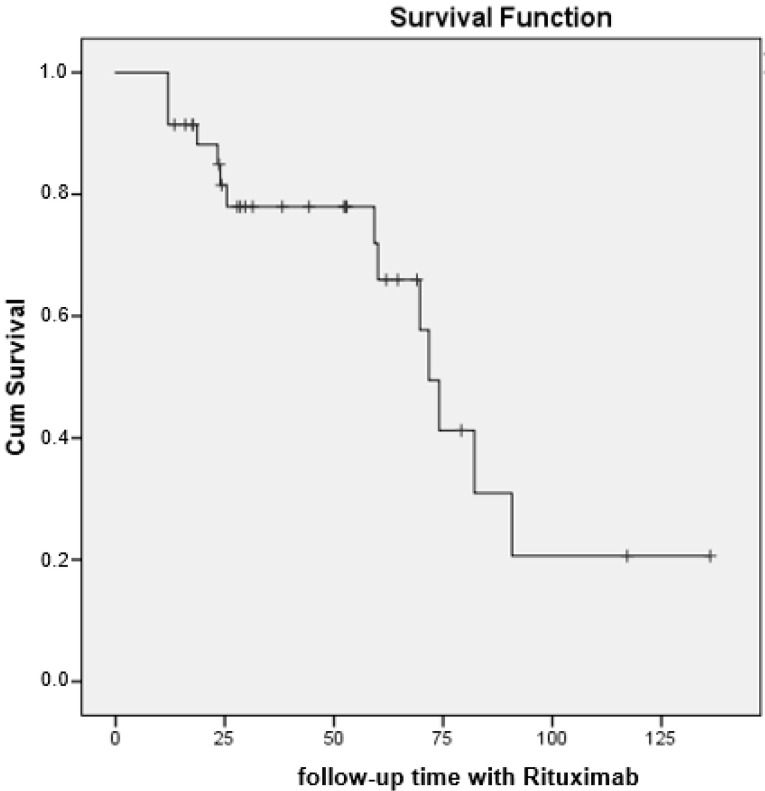
We included 37 patients with CTD-ILD treated with RTX for a median (IQR) of 38.2 (17.7-69.0) months. At the end of the follow-up, disease had improved or stabilized in 23 patients (62.1%) and worsened in seven (18.9%); seven patients (18.9%) died. No significant decline was observed in median FVC (72.2 vs. 70.8; = 0.530) or DLCO (55.9 vs. 52.2; = 0.100). The multivariate analysis showed the independent predictors for worsening of CTD-ILD to be baseline DLCO (OR (95% CI), 0.904 (0.8-0.9); = 0.015), time to initiation of RTX (1.01 (1.001-1.02); = 0.029), and mycophenolate (0.202 (0.04-0.8); = 0.034). Only 28 of the 37 patients (75.6%) were still undergoing treatment with RTX: two patients (5.4%) stopped treatment due to adverse events and seven patients (18.9%) died owing to progression of ILD and superinfection.
Lung function improved or stabilized in more than half of patients with CTD-ILD treated with RTX. Early treatment and combination with mycophenolate could reduce the risk of progression of ILD.
分析利妥昔单抗(RTX)治疗结缔组织病相关间质性肺病(CTD-ILD)的疗效及安全性。
我们对2015年至2020年间接受利妥昔单抗治疗的CTD-ILD患者进行了一项多中心、前瞻性观察性研究。在基线、12个月及随访结束时,使用高分辨率计算机断层扫描和肺功能测试对患者进行评估。随访结束时的主要结局指标为用力肺活量(FVC)增加>10%或肺一氧化碳弥散量(DLCO)增加>15%,以及影像学进展或死亡。我们记录了临床特征、开始RTX治疗的时间、联合治疗、感染及住院情况。进行Cox回归分析以确定与ILD恶化相关的因素。
我们纳入了37例接受RTX治疗的CTD-ILD患者,治疗时间中位数(IQR)为38.2(17.7-69.0)个月。随访结束时,23例患者(62.1%)病情改善或稳定,7例患者(18.9%)病情恶化;7例患者(18.9%)死亡。FVC中位数(72.2对70.8;P = 0.530)或DLCO中位数(55.9对52.2;P = 0.100)未观察到显著下降。多因素分析显示,CTD-ILD恶化的独立预测因素为基线DLCO(OR(95%CI),0.904(0.8-0.9);P = 0.015)、开始RTX治疗的时间(1.01(1.001-1.02);P = 0.029)及霉酚酸酯(0.202(0.04-0.8);P = 0.034)。37例患者中仅28例(75.6%)仍在接受RTX治疗:2例患者(5.4%)因不良事件停止治疗,7例患者(18.9%)因ILD进展和重叠感染死亡。
接受RTX治疗的CTD-ILD患者中,超过半数患者的肺功能得到改善或稳定。早期治疗及联合霉酚酸酯可降低ILD进展风险。