Chen Guangyong, Ren Junli, Huang Honghao, Shen Jiamin, Yang Chenguang, Hu Jingyu, Pan Wenjing, Sun Fangyue, Zhou Xinbo, Zeng Tian, Li Shengqi, Yang Dehao, Weng Yiyun
Department of Neurology, The Third Affiliated Hospital of Wenzhou Medical University, Wenzhou, China.
School of the First Clinical Medical Sciences, Wenzhou Medical University, Wenzhou, China.
Front Aging Neurosci. 2022 Feb 8;14:782282. doi: 10.3389/fnagi.2022.782282. eCollection 2022.
Stress hyperglycemia ratio (SHR), calculated as glucose/glycated hemoglobin, has recently been developed for assessing stress hyperglycemia and could provide prognostic information for various diseases. However, calculating SHR using random blood glucose (RBG) drawn on admission or fasting blood glucose (FBG) could lead to different results. This study intends to evaluate the association between SHR and functional outcomes in patients with acute ischemic stroke (AIS) with recombinant tissue plasminogen activator (r-tPA) intravenous thrombolysis.
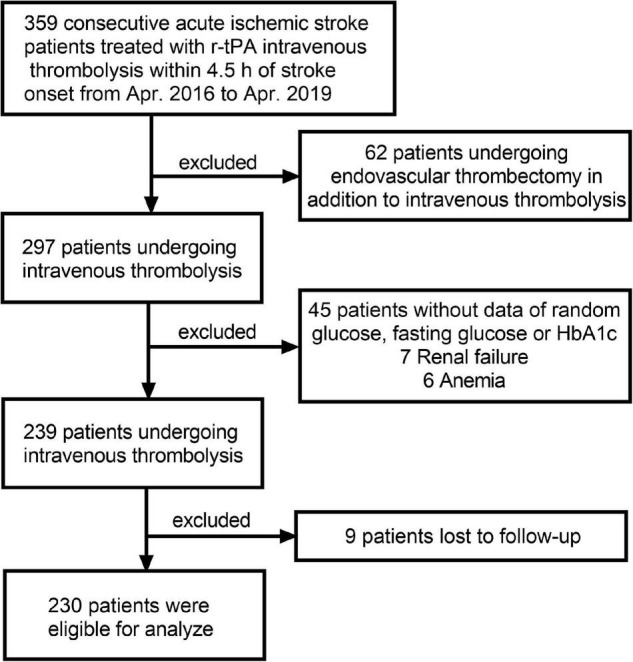
Data from 230 patients with AIS following thrombolytic therapy with r-tPA in the Third Affiliated Hospital of Wenzhou Medical University from April 2016 to April 2019 were retrospectively reviewed. SHR1 was defined as [RBG (mmol/L)]/[HbA1c (%)] and SHR2 was defined as [FBG (mmol/L)]/[HbA1c (%)]. The outcomes included early neurological improvement (ENI), poor function defined as a modified Rankin Scale score (mRS) of 3-6, and all-cause death in 3 months. Multivariable logistic regression was performed to estimate the association between SHR and adverse outcomes.
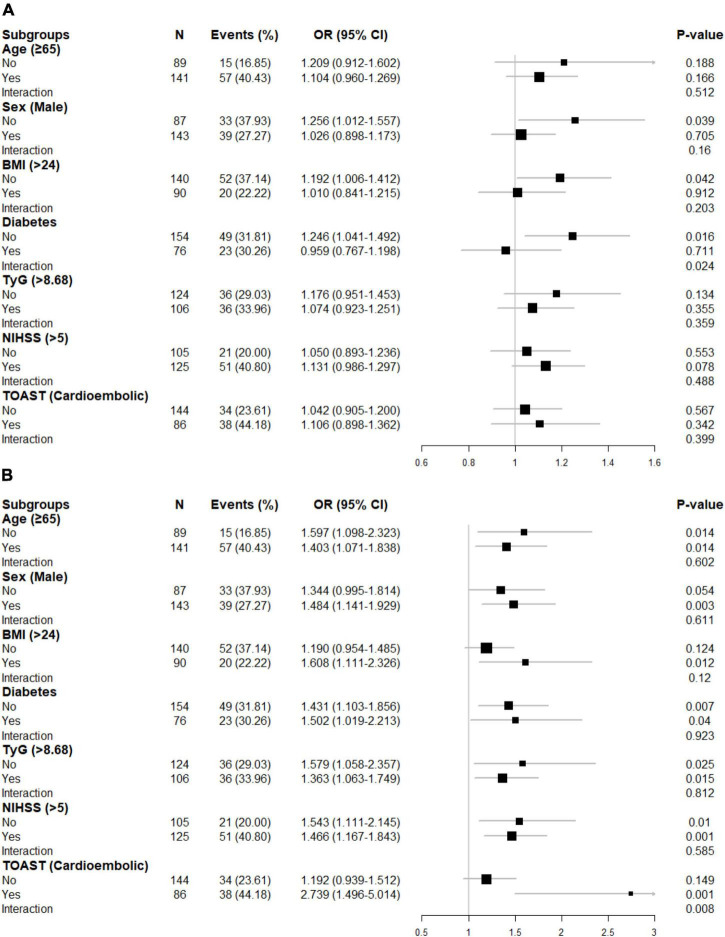
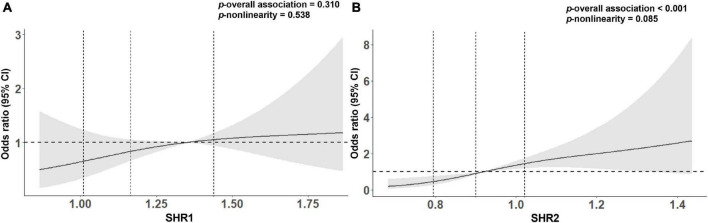
After adjustment for possible confounders, though patients with AIS with higher SHR1 tend to have a higher risk of poor outcome and death and unlikely to develop ENI, these did not reach the statistical significance. In contrast, SHR2 was independently associated with poor functional outcome (per 0.1-point increases: odds ratios (OR) = 1.383 95% CI [1.147-1.668]). Further adjusted for body mass index (BMI), triglyceride-glucose index (TyG), and diabetes slightly strengthen the association between SHR (both 1 and 2) and adverse outcomes. In subgroup analysis, elevated SHR1 is associated with poor functional outcomes (per 0.1-point increases: OR = 1.246 95% CI [1.041-1.492]) in non-diabetic individuals and the association between SHR2 and the poor outcomes was attenuated in non-cardioembolic AIS.
SHR is expected to replace random or fasting glucose concentration as a novel generation of prognostic indicator and a potential therapeutic target.
应激性高血糖比率(SHR),计算方式为血糖/糖化血红蛋白,最近已被开发用于评估应激性高血糖,并可为各种疾病提供预后信息。然而,使用入院时采集的随机血糖(RBG)或空腹血糖(FBG)计算SHR可能会导致不同结果。本研究旨在评估急性缺血性卒中(AIS)患者接受重组组织型纤溶酶原激活剂(r - tPA)静脉溶栓治疗时SHR与功能结局之间的关联。
回顾性分析了2016年4月至2019年4月在温州医科大学附属第三医院接受r - tPA溶栓治疗的230例AIS患者的数据。SHR1定义为[RBG(mmol/L)]/[糖化血红蛋白(%)],SHR2定义为[FBG(mmol/L)]/[糖化血红蛋白(%)]。结局包括早期神经功能改善(ENI)、改良Rankin量表评分(mRS)为3 - 6定义的功能不良以及3个月内的全因死亡。进行多变量逻辑回归以估计SHR与不良结局之间的关联。
在对可能的混杂因素进行调整后,尽管SHR1较高的AIS患者出现不良结局和死亡的风险往往较高,且不太可能出现ENI,但这些均未达到统计学意义。相比之下,SHR2与功能不良结局独立相关(每增加0.1分:比值比(OR)= 1.383,95%置信区间[1.147 - 1.668])。进一步对体重指数(BMI)、甘油三酯 - 血糖指数(TyG)和糖尿病进行调整后,略微增强了SHR(1和2)与不良结局之间的关联。在亚组分析中,非糖尿病个体中SHR1升高与功能不良结局相关(每增加0.1分:OR = 1.246,95%置信区间[1.041 - 1.492]),且在非心源性栓塞性AIS中SHR2与不良结局之间的关联减弱。
SHR有望取代随机或空腹血糖浓度,成为新一代的预后指标和潜在的治疗靶点。