Liang Jingjing, Zhang Lingyu, Huang Zhidong, He Yibo, Ling Yihang, Chen Kai, Ying Ming, Lin Mengfei, Li Guode, Liu Jin, Liu Yong, Liang Yan, Chen Shiqun, Hu Yunzhao
Department of Cardiology, Shunde Hospital, Southern Medical University, Foshan, China.
The Second School of Clinical Medicine, Southern Medical University, Guangzhou, China.
Front Nutr. 2022 Feb 8;8:795068. doi: 10.3389/fnut.2021.795068. eCollection 2021.
The relationship between malnutrition and the risk of contrast-associated acute kidney injury (CA-AKI) and the resulting prognosis in patients undergoing percutaneous coronary intervention (PCI) is still not well known.
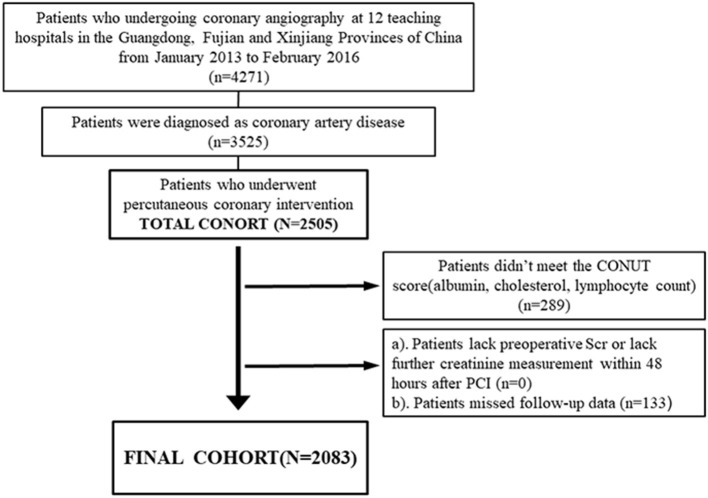
Patients undergoing PCI were consecutively enrolled in a multicenter study in China (NCT01402232), categorized by nutritional status (non-malnutrition, malnutrition) based on two different cut-off values (i.e., traditional threshold and the best cut-off value based on the receiver operating characteristic (ROC) curve) for the controlling nutritional status (CONUT) score. The primary endpoint was CA-AKI, diagnosed as a rise in serum creatinine >0.3 mg/dl or >50% than the baseline level occurring within 48 h after the intervention. The secondary endpoint was all-cause mortality. The relationships of malnutrition, CA-AKI, and all-cause mortality were examined using multivariate-adjusted logistic and Cox regression analyses, respectively.
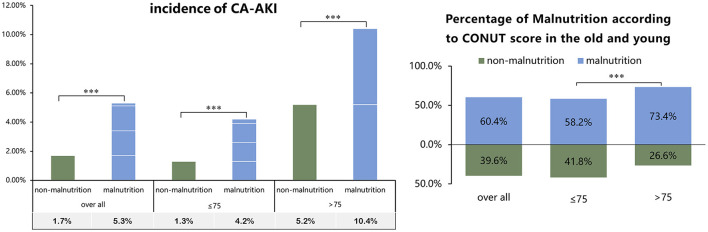
Among 2,083 patients undergoing PCI (age: 62.8 ± 11.1 years; 79.0% men), 1,258 (60.4%) were malnourished. During hospitalization, 80 (3.8%) patients developed CA-AKI events. The incidence of CA-AKI in patients who did not have malnutrition (the non-malnutrition group) and those who did have malnutrition (the malnutrition group) was 1.7% and 5.25%, respectively. Patients with malnutrition had a 2-fold increased adjusted risk of CA-AKI compared to those with no malnutrition [adjusted odds ratio (aOR) (95% confidence interval CI): 2.41 (1.22 to 5.22)]. Malnutrition was associated with a 3-fold increased adjusted risk of CA-AKI in patients aged ≤ 75 years [ = 1,791, aOR (95% CI): 3.39 (1.46-9.25)]. Malnourished patients with CA-AKI had a higher risk of all-cause mortality than the others. Similar results were observed in the grouping of Supplemental Analyses based on the optimal cut-off value of the CONUT score identified by the ROC curve.
Malnutrition is strongly associated with an increased risk of CA-AKI in both young and old patients undergoing PCI. Malnourished patients with CA-AKI had a significantly higher risk of all-cause mortality. Further studies are needed to prospectively assess the efficacy of nutritional interventions on outcomes in patients undergoing PCI.
营养不良与接受经皮冠状动脉介入治疗(PCI)患者的对比剂相关急性肾损伤(CA-AKI)风险及预后之间的关系仍未完全明确。
在中国一项多中心研究(NCT01402232)中连续纳入接受PCI的患者,根据控制营养状况(CONUT)评分的两个不同临界值(即传统阈值和基于受试者工作特征曲线(ROC)的最佳临界值)将患者按营养状况分类(非营养不良、营养不良)。主要终点为CA-AKI,定义为干预后48小时内血清肌酐升高>0.3mg/dl或比基线水平升高>50%。次要终点为全因死亡率。分别采用多变量调整逻辑回归和Cox回归分析来研究营养不良、CA-AKI和全因死亡率之间的关系。
在2083例接受PCI的患者中(年龄:62.8±11.1岁;男性占79.0%),1258例(60.4%)存在营养不良。住院期间,80例(3.8%)患者发生CA-AKI事件。无营养不良患者(非营养不良组)和有营养不良患者(营养不良组)的CA-AKI发生率分别为1.7%和5.25%。与无营养不良患者相比,营养不良患者发生CA-AKI的调整后风险增加2倍[调整优势比(aOR)(95%置信区间CI):2.41(1.22至5.22)]。在年龄≤75岁的患者中,营养不良与CA-AKI的调整后风险增加3倍相关[ = 1791,aOR(95%CI):3.39(1.46 - 9.25)]。发生CA-AKI的营养不良患者全因死亡风险高于其他患者。在基于ROC曲线确定的CONUT评分最佳临界值进行的补充分析分组中也观察到了类似结果。
在接受PCI的老年和年轻患者中,营养不良与CA-AKI风险增加密切相关。发生CA-AKI的营养不良患者全因死亡风险显著更高。需要进一步研究前瞻性评估营养干预对接受PCI患者结局的疗效。