Zeng Ji-Lang, Xiang Yi-Fei, Zhang Li-Wei, Chen Li-Chuan, Chen Jun-Han, Liang Wen-Jia, You Zhebin, Wang Chang-Xi, Lin Zhi-Jie, Lin Kai-Yang, Guo Yansong
Department of Cardiology, Shengli Clinical Medical College of Fujian Medical University, Fujian Provincial Hospital, Fuzhou, People's Republic of China.
Fujian Provincial Key Laboratory of Cardiovascular Disease, Fujian Provincial Center for Geriatrics, Fujian Provincial Clinical Research Center for Severe Acute Cardiovascular Diseases, Fuzhou, People's Republic of China.
J Inflamm Res. 2023 Jul 8;16:2845-2854. doi: 10.2147/JIR.S419831. eCollection 2023.
Prior research has demonstrated a key role of systemic inflammatory state in the pathogenesis and progression of contrast-associated acute kidney injury (CA-AKI). Recently, the systemic inflammation score (SIS) has been introduced to evaluate the inflammatory status, utilizing the lymphocyte-to-monocyte ratio (LMR) and albumin. The primary objective of this study was to determine whether the SIS can predict CA-AKI and long-term prognosis in patients undergoing elective percutaneous coronary intervention (PCI).
A total of 5726 patients who underwent elective PCI were included from January 2012 to December 2018. The primary outcome was CA-AKI, defined as an increase in serum creatinine (SCr) ≥0.3 mg/dl or ≥50% than baseline SCr within 48 h after the PCI procedure. The secondary outcome was long-term mortality. All patients were classified into low- and high-SIS groups.
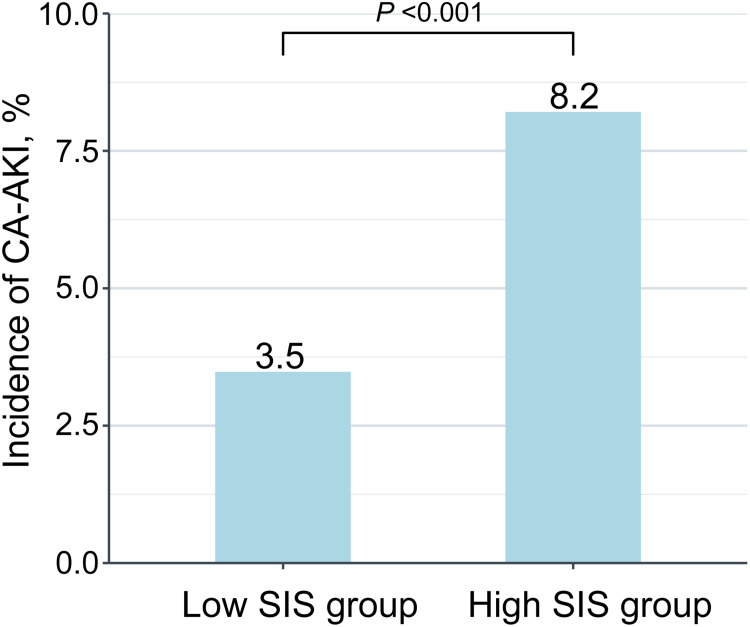
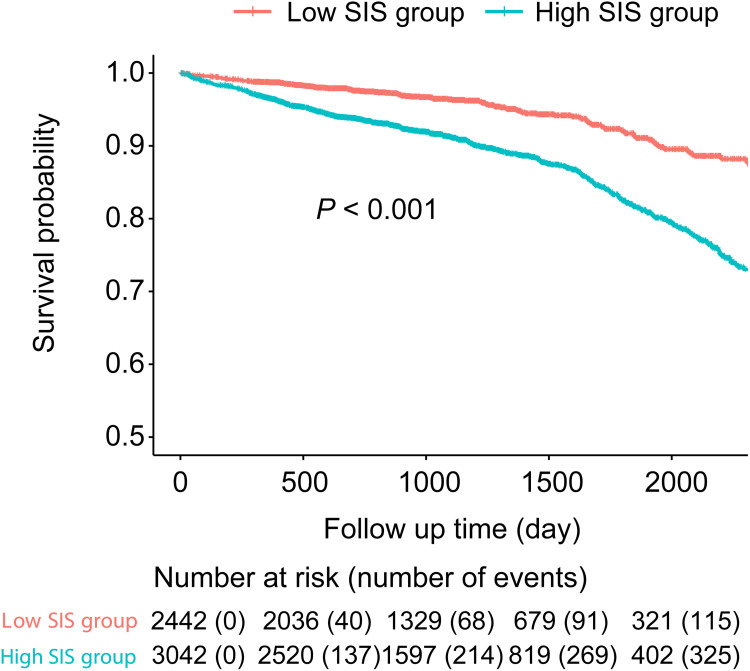
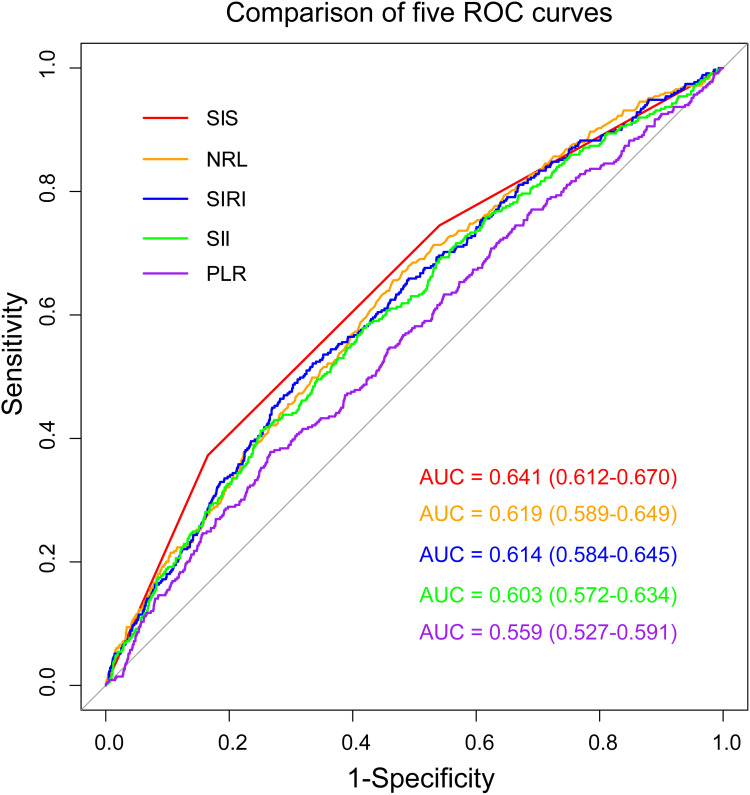
During hospitalization, 349 (6.1%) patients developed CA-AKI. Multivariate logistic regression analysis showed that patients in the high SIS group had a 1.47-fold higher risk of developing CA-AKI than those in the low SIS group [odds ratio (OR): 1.50, 95% confidence interval (CI): 1.12-2.01, =0.006]. Furthermore, the SIS showed the greatest prediction performance for CA-AKI compared with other inflammatory hematological ratios. In the multivariate Cox regression analysis, the high SIS group was found to be closely associated with long-term mortality [hazard ratio (HR): 1.58, 95% CI: 1.26-1.97, <0.001, vs low SIS group]. The Kaplan-Meier curve analysis also demonstrated a difference in long-term mortality between the two groups (Log rank test, <0.001).
The SIS was closely associated with CA-AKI and long-term mortality in patients after elective PCI. Thus, more attention should be paid to exploring the potential benefits of anti-inflammatory strategies in preventing CA-AKI and improving the prognosis of patients undergoing PCI.
先前的研究已证明全身炎症状态在造影剂相关性急性肾损伤(CA-AKI)的发病机制和进展中起关键作用。最近,全身炎症评分(SIS)已被引入以评估炎症状态,该评分利用淋巴细胞与单核细胞比值(LMR)和白蛋白。本研究的主要目的是确定SIS是否能够预测接受择期经皮冠状动脉介入治疗(PCI)患者的CA-AKI及长期预后。
纳入2012年1月至2018年12月期间接受择期PCI的5726例患者。主要结局为CA-AKI,定义为PCI术后48小时内血清肌酐(SCr)升高≥0.3mg/dl或较基线SCr升高≥50%。次要结局为长期死亡率。所有患者被分为低SIS组和高SIS组。
住院期间,349例(6.1%)患者发生CA-AKI。多因素逻辑回归分析显示,高SIS组患者发生CA-AKI的风险比低SIS组高1.47倍[比值比(OR):1.50,95%置信区间(CI):1.12 - 2.01,P = 0.006]。此外,与其他炎症血液学比值相比,SIS对CA-AKI的预测性能最佳。在多因素Cox回归分析中,发现高SIS组与长期死亡率密切相关[风险比(HR):1.58,95% CI:1.26 - 1.97,P < 0.001,与低SIS组相比]。Kaplan-Meier曲线分析也显示两组之间长期死亡率存在差异(对数秩检验,P < 0.001)。
SIS与择期PCI术后患者的CA-AKI及长期死亡率密切相关。因此,应更加关注探索抗炎策略在预防CA-AKI和改善PCI患者预后方面的潜在益处。