Stassen Jan, Galloo Xavier, Chimed Surenjav, Hirasawa Kensuke, Marsan Nina Ajmone, Delgado Victoria, van der Bijl Pieter, Bax Jeroen J
Department of Cardiology, Leiden University Medical Center, Albinusdreef 2, 2300 RC Leiden, The Netherlands.
Department of Cardiology, Jessa Hospital, 3500 Hasselt, Belgium.
Eur Heart J Cardiovasc Imaging. 2022 Jun 1;23(6):730-740. doi: 10.1093/ehjci/jeac042.
Left atrial (LA) function is a marker of prognosis in patients with heart failure. The prognostic implications of an improvement in LA function in addition to an improvement in left ventricular (LV) function after cardiac resynchronization therapy (CRT) implantation are unknown. This study aimed to evaluate the prognostic value of a significant change in LA reservoir strain (RS) and/or LV global longitudinal strain (GLS) after initiation of CRT.
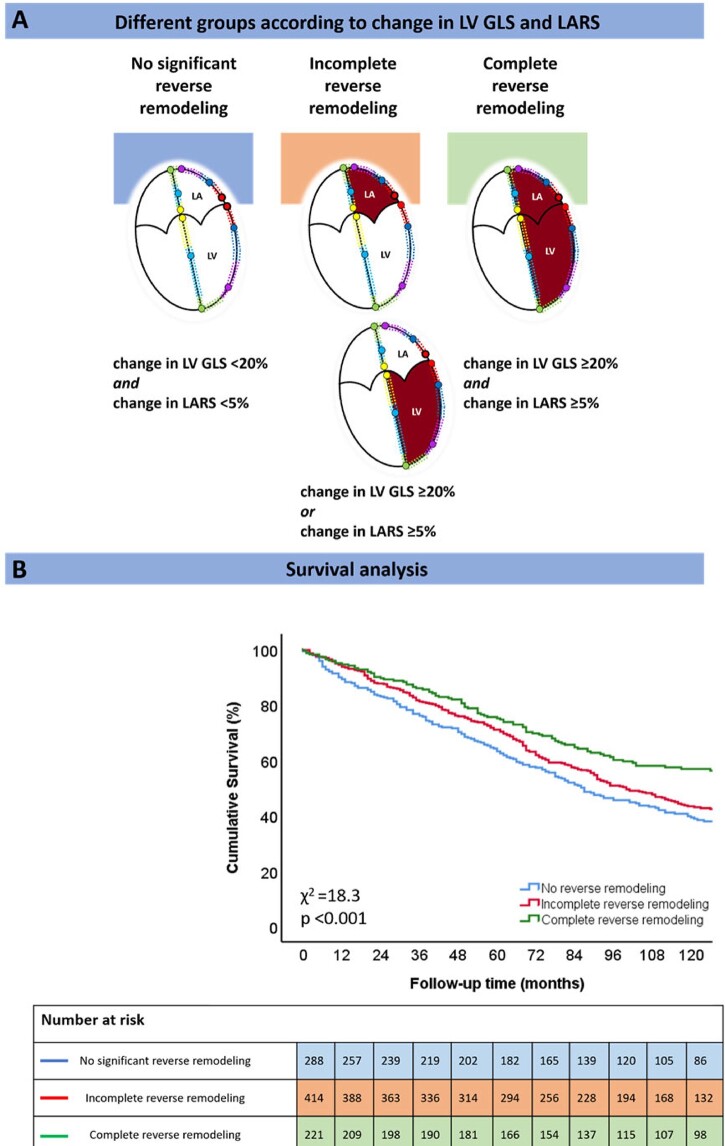
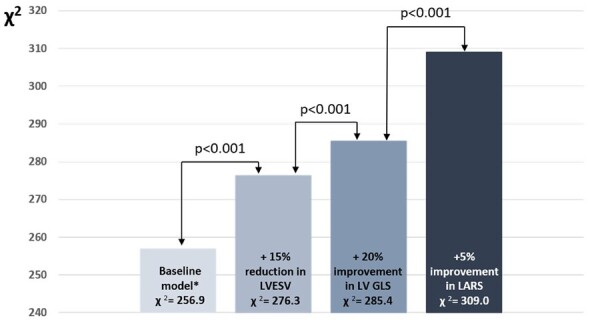
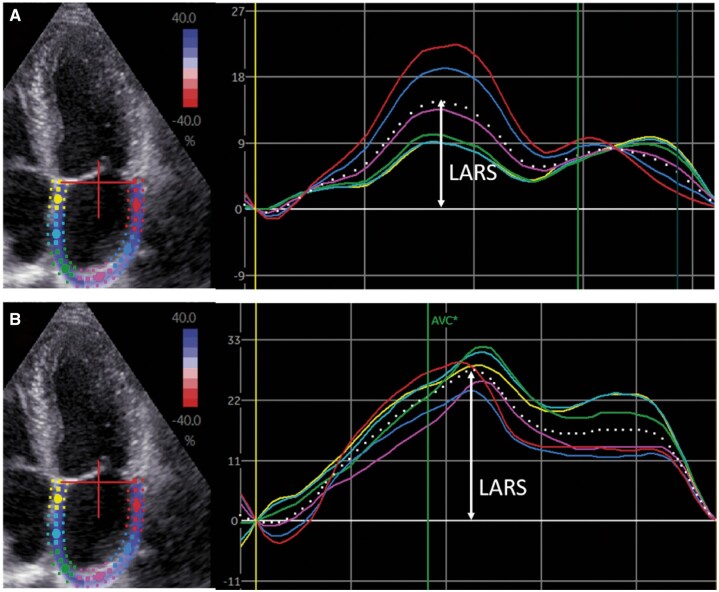
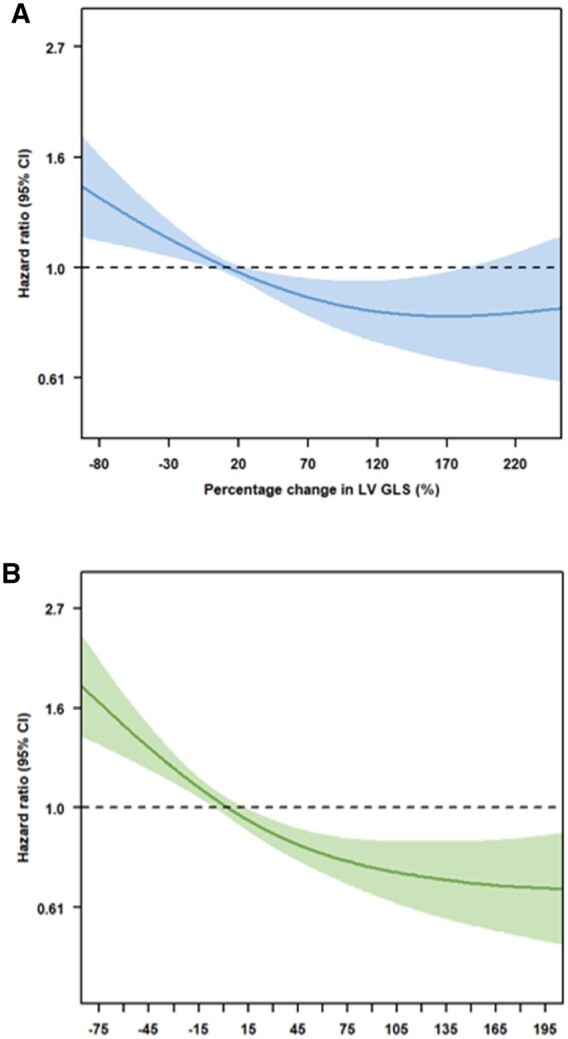
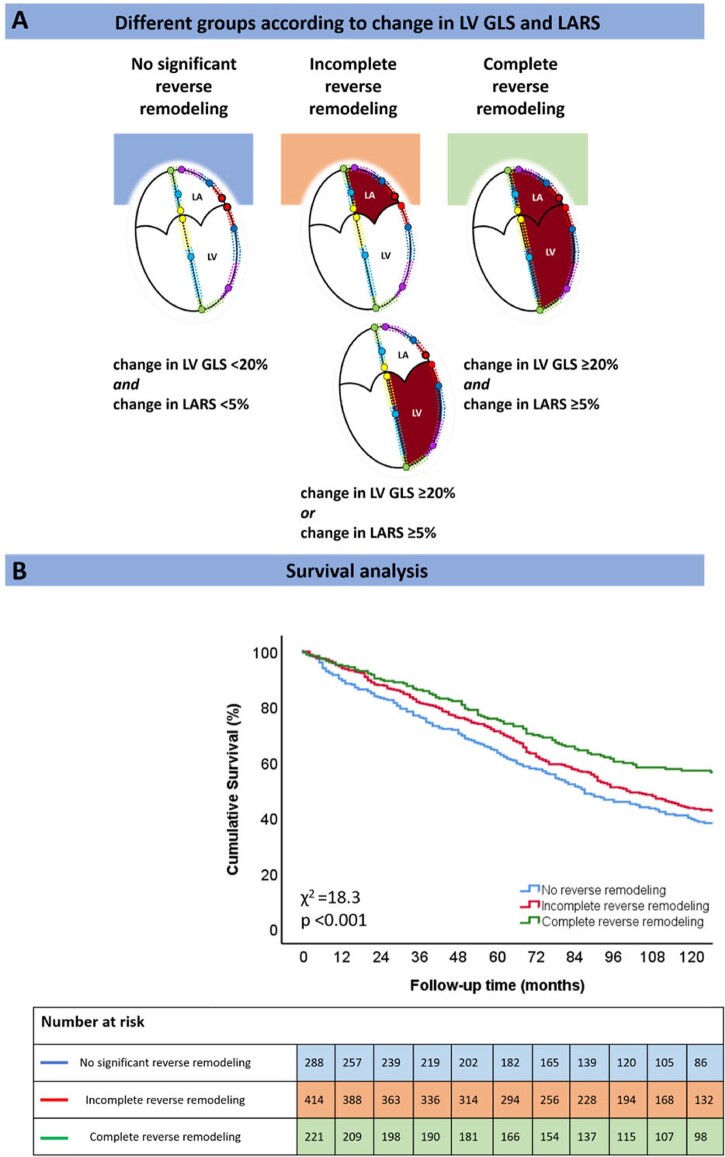
LARS and LVGLS were measured with speckle-tracking echocardiography. Significant improvement in LARS and LVGLS was defined as a percentage change of +5% and +20% at 6 months after CRT implantation, respectively. Patients were divided into three groups: no significant reverse remodelling (no improvement in LARS and LVGLS), incomplete reverse remodelling (improvement in LARS or LVGLS), and complete reverse remodelling (improvement in LARS and LVGLS). The primary endpoint was all-cause mortality. A total of 923 patients (mean age 65 ± 10 years, 77% male) were included, of which 221 (24%) had complete reverse remodelling, 414 (45%) incomplete reverse remodelling, and 288 (31%) no significant reverse remodelling. Five-years' mortality was 24%, 29%, and 36% for patients with complete, incomplete, and no significant reverse remodelling, respectively (P < 0.001). On multivariable analysis, complete reverse remodelling (hazard ratio 0.477; 95% confidence interval: 0.362-0.628; P < 0.001) was associated with the lowest risk of mortality.
Patients with complete reverse remodelling have a lower mortality risk than those showing incomplete or no significant reverse remodelling. The use of integrated LA and LV deformation imaging may improve risk-stratification of CRT recipients.
左心房(LA)功能是心力衰竭患者预后的一个指标。心脏再同步治疗(CRT)植入后,除左心室(LV)功能改善外,LA功能改善的预后意义尚不清楚。本研究旨在评估CRT开始后LA储备应变(RS)和/或LV整体纵向应变(GLS)的显著变化的预后价值。
用斑点追踪超声心动图测量LARS和LVGLS。LARS和LVGLS的显著改善分别定义为CRT植入后6个月时变化百分比为+5%和+20%。患者分为三组:无显著逆向重构(LARS和LVGLS无改善)、不完全逆向重构(LARS或LVGLS改善)和完全逆向重构(LARS和LVGLS改善)。主要终点是全因死亡率。共纳入923例患者(平均年龄65±10岁,77%为男性),其中221例(24%)有完全逆向重构,414例(45%)有不完全逆向重构,288例(31%)无显著逆向重构。完全、不完全和无显著逆向重构患者的五年死亡率分别为24%、29%和36%(P<0.001)。多变量分析显示,完全逆向重构(风险比0.477;95%置信区间:0.362 - 0.628;P<0.001)与最低死亡风险相关。
完全逆向重构的患者比不完全或无显著逆向重构的患者有更低的死亡风险。综合使用LA和LV形变成像可能改善CRT接受者的风险分层。