Asthma Research Group Windsor-Essex County Inc., Windsor, ON, Canada.
London School of Hygiene and Tropical Medicine, London, UK.
Int J Chron Obstruct Pulmon Dis. 2021 Dec 22;16:3449-3464. doi: 10.2147/COPD.S338851. eCollection 2021.
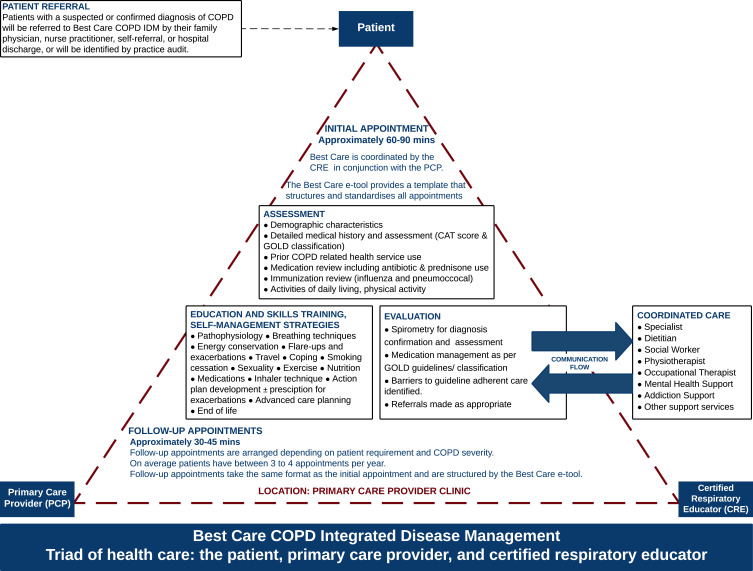
Integrated disease management (IDM) for COPD in primary care has been primarily investigated under clinical trial conditions. We previously published a randomized controlled trial (RCT) where the IDM intervention improved quality of life (QoL) and exacerbation-related outcomes. In this study, we assess the same IDM intervention in a real-world evaluation and identify patient characteristics associated with improved outcomes.
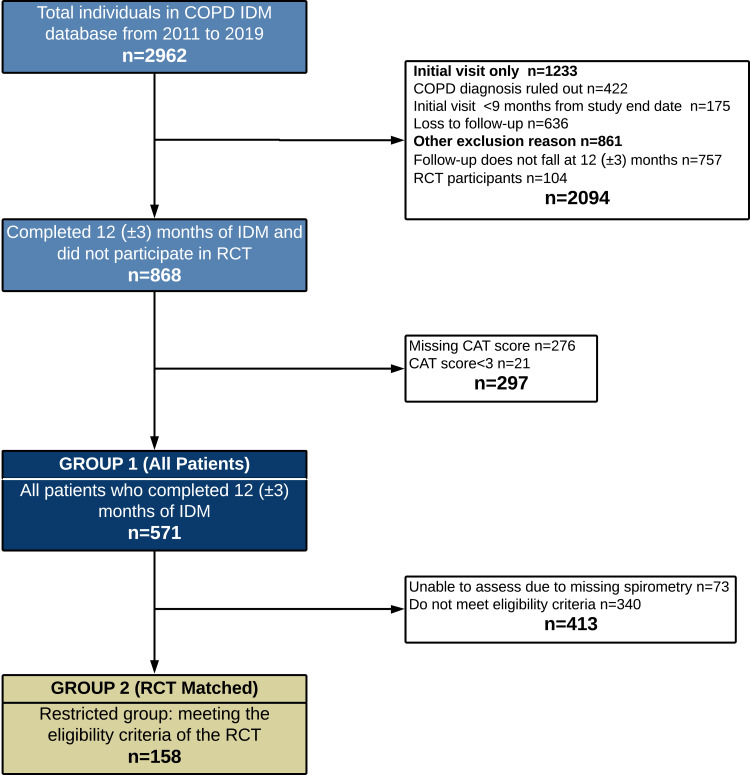
This historical cohort study included patients enrolled for 12 (±3 months) in the Best Care COPD IDM program. The main outcome was a ≥3 point improvement in COPD assessment test (CAT). Secondary outcomes were COPD exacerbations requiring antibiotics and/or prednisone, unscheduled physician visits, emergency department visits and hospitalizations.
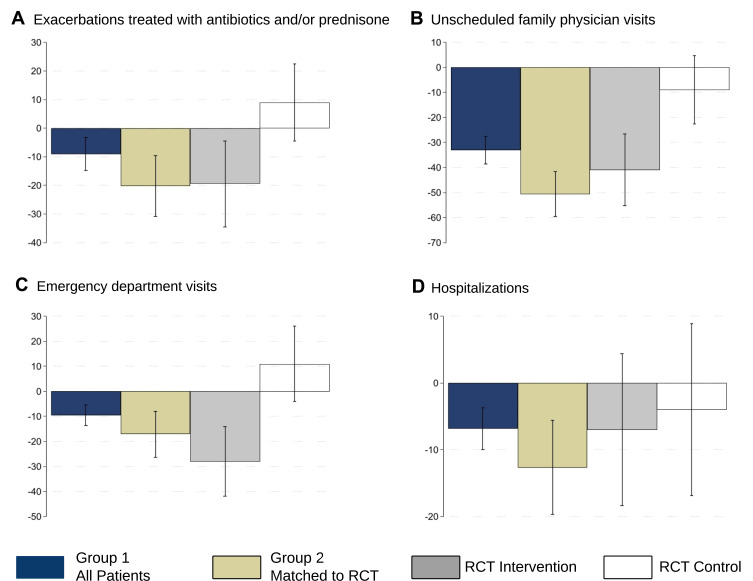
Data for 571 patients ( were included, 158 met the reference RCT eligibility . Improved QoL was observed in 43% (95% CI:38.9,47.2) of , 47% (95% CI:39.5,55.6) of vs 92% (95% CI:79.2,95.1) in the reference RCT intervention arm (n=72). Reductions (12 months IDM vs prior year) were observed in the proportion of patients experiencing exacerbation-related events (): antibiotics/prednisone (-9.0%,95% CI:-13.9,-3.9); unscheduled physician (-33.1%,95% CI:-38.2,-27.9); emergency department (-9.6%,95% CI:-13.5,-5); and hospitalizations (-6.8%,95% CI:-10.0,-3.7). For the all reductions were comparable to the reference RCT intervention arm. The strongest predictors of improved QoL were baseline CAT, CAT≥20 vs CAT<10 (OR 15.6,95% CI:7.91,30.83), GOLD group B (OR 6.4,95% CI:3.42,11.85) and D (OR 5.64,95% CI:2.80,11.37) vs GOLD group A. Patients with prior antibiotic/prednisone use, FEV <30% predicted and GOLD group D were less likely to have no urgent health service utilization (OR 0.5,95% CI:0.30,0.68), (OR 0.2,95% CI:0.07,0.78) and (OR 0.3,95% CI:0.14,0.51), respectively.
Best Care COPD improved QoL and reduced exacerbation-related outcomes in a manner directionally similar to the RCT from which it emanated. Baseline QoL, exacerbation history, and GOLD category were identified as possible predictors of IDM impact and will inform future program development and resource allocation.
在初级保健中,综合疾病管理(IDM)对 COPD 的治疗主要在临床试验条件下进行了研究。我们之前发表了一项随机对照试验(RCT),其中 IDM 干预措施改善了生活质量(QoL)和与加重相关的结局。在本研究中,我们在真实世界评估中评估了相同的 IDM 干预措施,并确定了与改善结局相关的患者特征。
这项历史队列研究纳入了在 Best Care COPD IDM 计划中登记了 12(±3 个月)的患者。主要结局是 COPD 评估测试(CAT)至少改善 3 分。次要结局是需要抗生素和/或泼尼松治疗的 COPD 加重、非计划就诊、急诊就诊和住院治疗。
共纳入 571 例患者()的数据,其中 158 例符合参考 RCT 的入选标准。与参考 RCT 干预组(n=72)相比,95%CI:38.9,47.2)的()中,有 43%(95%CI:38.9,47.2)的患者 QoL 得到改善,有 47%(95%CI:39.5,55.6)的患者 QoL 得到改善。与前一年相比,经历加重相关事件的患者比例有所下降():抗生素/泼尼松(-9.0%,95%CI:-13.9,-3.9);非计划就诊(-33.1%,95%CI:-38.2,-27.9);急诊就诊(-9.6%,95%CI:-13.5,-5)和住院治疗(-6.8%,95%CI:-10.0,-3.7)。对于所有患者,这些减少与参考 RCT 干预组相当。改善 QoL 的最强预测因素是基线 CAT、CAT≥20 与 CAT<10(OR 15.6,95%CI:7.91,30.83)、GOLD 组 B(OR 6.4,95%CI:3.42,11.85)和 D(OR 5.64,95%CI:2.80,11.37)与 GOLD 组 A。有抗生素/泼尼松使用史、FEV<30%预计值和 GOLD 组 D 的患者更不可能有紧急卫生服务利用(OR 0.5,95%CI:0.30,0.68)、(OR 0.2,95%CI:0.07,0.78)和(OR 0.3,95%CI:0.14,0.51)。
Best Care COPD 以与 RCT 相似的方向改善了 QoL 并减少了与加重相关的结局。基线 QoL、加重史和 GOLD 分类被确定为 IDM 影响的可能预测因素,并将为未来的项目开发和资源分配提供信息。