Adams Elisabeth J, van Doornewaard Alexander, Ma Yixuan, Ahmed Nurilign, Cheng Man Ki, Watz Henrik, Ichinose Masakazu, Wilkinson Tom, Bhutani Mohit, Licskai Christopher J, Turner Katy M E
Aquarius Population Health, London, UK.
Pulmonary Research Institute at Lungen Clinic Grosshansdorf, Airway Research Center North (ARCN), German Center for Lung Research (DZL), Grosshansdorf, Germany.
Int J Chron Obstruct Pulmon Dis. 2023 Sep 27;18:2127-2146. doi: 10.2147/COPD.S416988. eCollection 2023.
COPD is a leading cause of morbidity and mortality globally. Management is complex and costly. Although international quality standards for diagnosis and management exist, opportunities remain to improve outcomes, especially in reducing avoidable hospitalisations.
To estimate the potential health and economic impact of improved adherence to guideline-recommended care for prevalent, on-treatment COPD populations in four high-income settings.
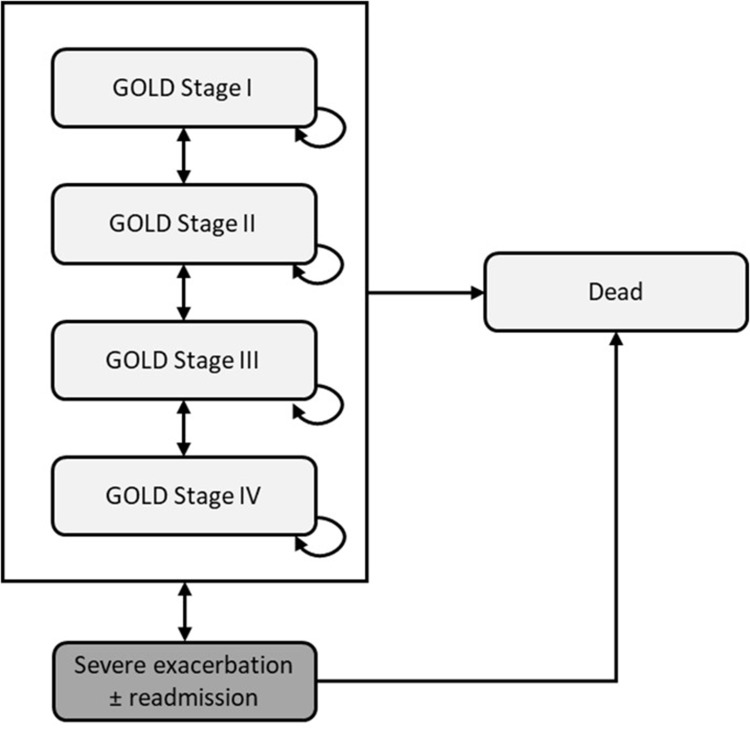
A disease simulation model was developed to evaluate the impact of theoretical improvements to COPD management, comparing outcomes for usual care and policy scenarios for interventions that reduce avoidable hospitalisations: 1) increased attendance (50% vs 31-38%) of early follow-up review after severe exacerbation hospitalisation; 2) increased access (30% vs 5-10%) to an integrated disease management (IDM) programme that provides guideline adherent care.
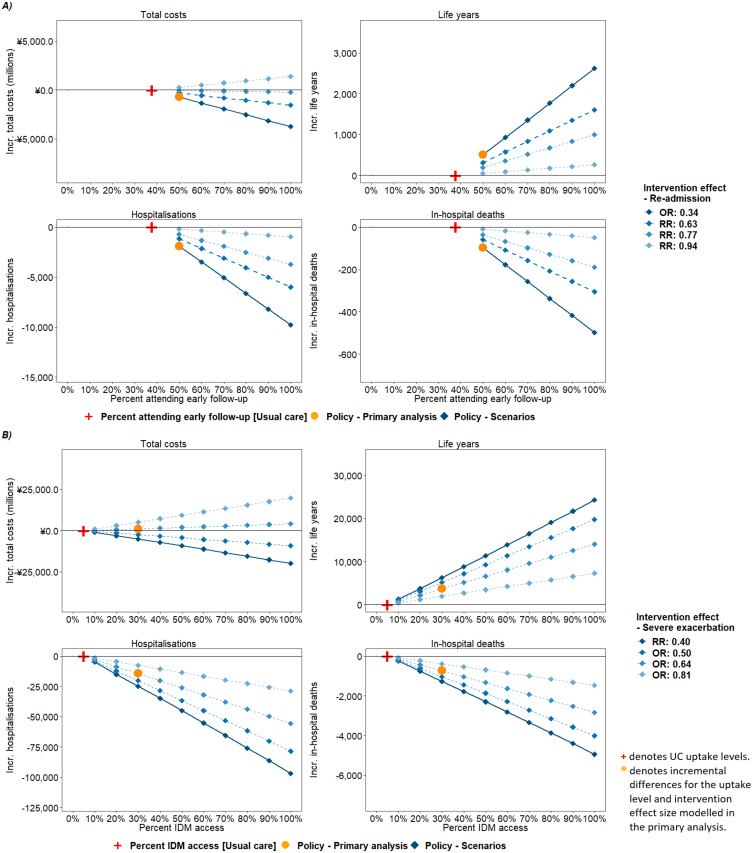
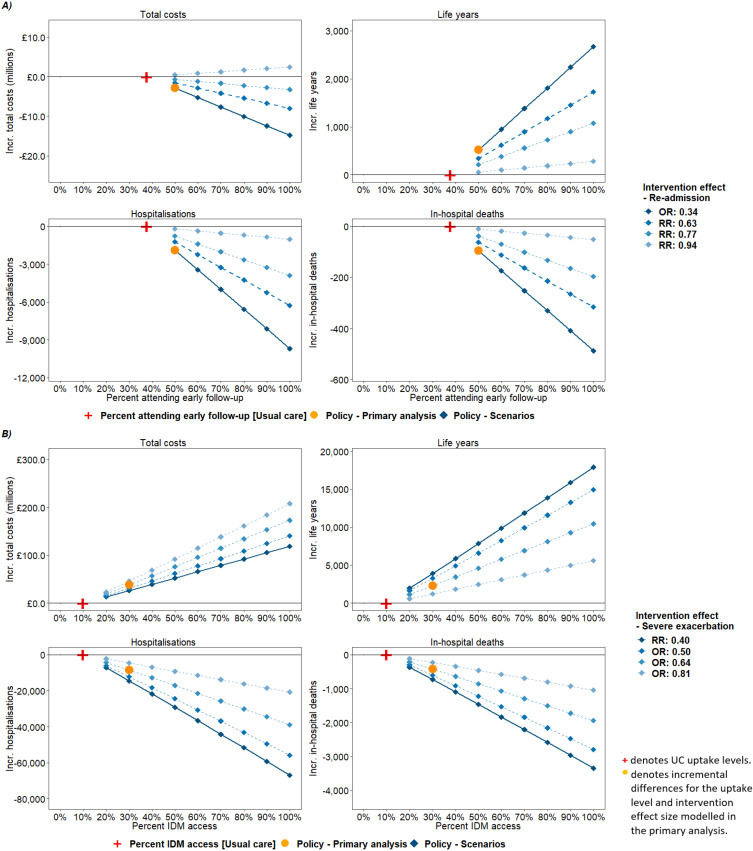
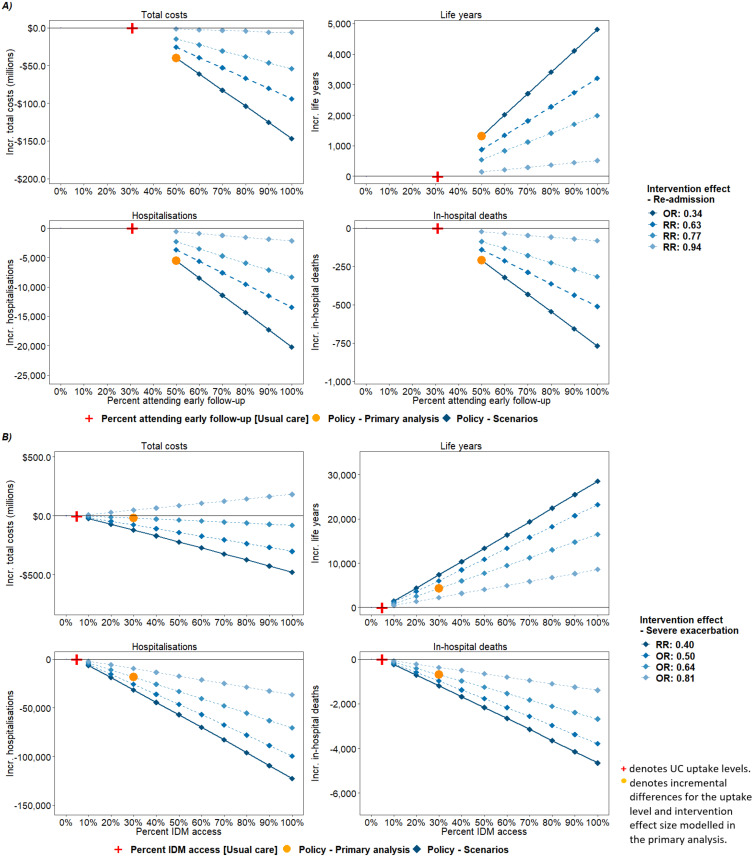
For cohorts of 100,000 patients, Policy 1 yielded additional life years (England: 523; Germany: 759; Canada: 1316; Japan: 512) and lifetime cost savings (-£2.89 million; -€6.58 million; -$40.08 million; -¥735.58 million). For Policy 2, additional life years (2299; 3619; 3656) and higher lifetime total costs (£38.15 million; €35.58 million; ¥1091.53 million) were estimated in England, Germany and Japan, and additional life years (4299) and cost savings (-$20.52 million) in Canada. Scenarios found that the cost impact depended on the modelled intervention effect size.
Interventions that reduce avoidable hospitalisations are estimated to improve survival and may generate cost savings. This study provides evidence on the theoretical impact of policies to improve COPD care and highlights priority areas for further research to support evidence-based policy decisions.
慢性阻塞性肺疾病(COPD)是全球发病和死亡的主要原因。其管理复杂且成本高昂。尽管存在诊断和管理的国际质量标准,但仍有改善结局的机会,尤其是在减少可避免的住院方面。
评估在四个高收入环境中,改善对指南推荐的治疗方案的依从性对现患、正在接受治疗的COPD人群的潜在健康和经济影响。
开发了一个疾病模拟模型,以评估COPD管理理论改进的影响,比较常规治疗和减少可避免住院的干预措施的政策情景的结果:1)严重加重住院后早期随访复查的就诊率增加(50%对31 - 38%);2)综合疾病管理(IDM)计划的可及性增加(30%对5 - 10%),该计划提供符合指南的护理。
对于100,000名患者的队列,政策1产生了额外的生命年(英国:523;德国:759;加拿大:1316;日本:512)和终身成本节约(-289万英镑;-658万欧元;-4008万美元;-7.3558亿日元)。对于政策2,在英国、德国和日本估计有额外的生命年(2299;3619;3656)和更高的终身总成本(3815万英镑;3558万欧元;10.9153亿日元),在加拿大有额外的生命年(4299)和成本节约(-2052万美元)。情景分析发现成本影响取决于模拟的干预效果大小。
估计减少可避免住院的干预措施可改善生存率并可能产生成本节约。本研究提供了关于改善COPD护理政策的理论影响的证据,并突出了进一步研究以支持基于证据的政策决策的优先领域。