Venugopal Anand, Carethers John M
Division of Gastroenterology and Hepatology, Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan, USA.
Department of Human Genetics and Rogel Cancer Center, University of Michigan, Ann Arbor, Michigan, USA.
EXCLI J. 2022 Jan 7;21:162-182. doi: 10.17179/excli2021-4456. eCollection 2022.
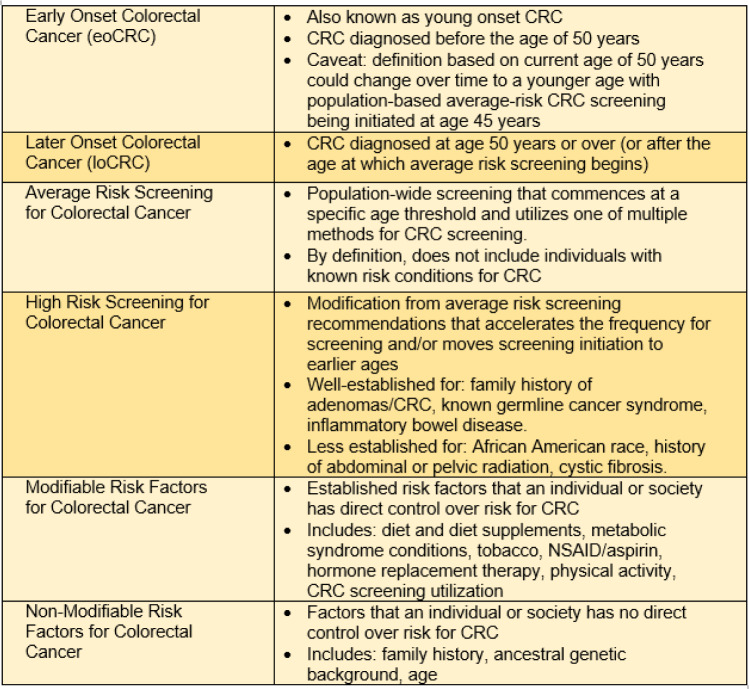
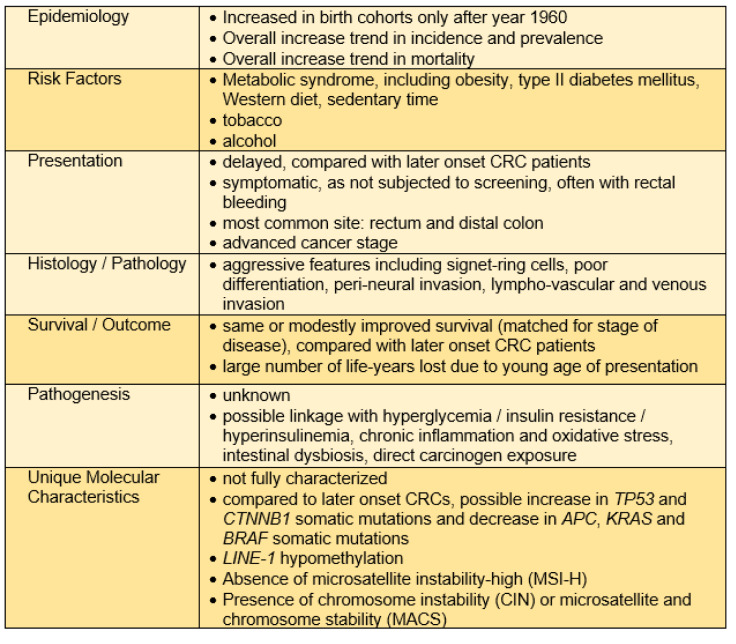
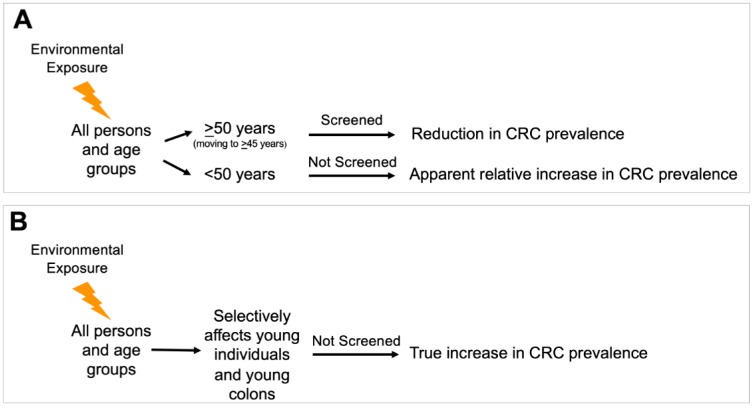
Colorectal cancer (CRC) is the third leading cause of cancer-related mortality in men or women in the United States. Average-risk screening that begins at age 50 years has reduced incidence and mortality of CRC in those over 50 years of age, whereas CRC incidence in those under age 50 years (early onset colorectal cancer (eoCRC)) has recently and dramatically increased. In this review, we summarize the recent literature including risk factors for eoCRC, differences in clinicopathologic presentation and outcomes in eoCRC, and emerging evidence regarding the molecular pathways that are altered in eoCRC compared to later onset CRC (loCRC). Epidemiologic studies of eoCRC show predominance in distal colon and rectum, and association with several modifiable risk factors, including diabetes, obesity, diet, sedentary time, alcohol consumption and smoking. Data regarding potential risk factors of prior antibiotic exposure and microbiome alterations or direct carcinogen exposure are still emerging. Aggressive clinicopathologic features of eoCRC at presentation may be due to delay in diagnosis or more aggressive tumor biology. EoCRC outcomes are similar to loCRC when matched for stage, but overall mortality is greater due to higher frequency of advanced disease at a younger presentation, with more life-years lost. There are only few molecular evaluations of eoCRC to date, with findings of potential increase in and somatic mutation and decrease in , and somatic mutation, compared to loCRC. Other findings include LINE-1 hypomethylation, absence of microsatellite instability (MSI-H), presence of chromosomal instability (CIN) or microsatellite and chromosomal stability (MACS). These studies are only now emerging and have not yet identified a specific molecular signature defining eoCRC. Further research evaluating genetic and molecular differences as well as environmental triggers for eoCRCs should provide a clearer understanding to inform targeted screening for pre-symptomatic at-risk younger individuals.
结直肠癌(CRC)是美国男性和女性癌症相关死亡的第三大主要原因。50岁开始的平均风险筛查降低了50岁以上人群中CRC的发病率和死亡率,而50岁以下人群(早发性结直肠癌(eoCRC))的CRC发病率最近却急剧上升。在本综述中,我们总结了近期的文献,包括eoCRC的危险因素、eoCRC临床病理表现和结局的差异,以及与晚发性结直肠癌(loCRC)相比,eoCRC中发生改变的分子途径的新证据。eoCRC的流行病学研究表明,其在远端结肠和直肠中占主导地位,并与多种可改变的危险因素相关,包括糖尿病、肥胖、饮食、久坐时间、饮酒和吸烟。关于先前抗生素暴露、微生物群改变或直接致癌物暴露等潜在危险因素的数据仍在不断涌现。eoCRC在初诊时具有侵袭性的临床病理特征可能是由于诊断延迟或肿瘤生物学行为更具侵袭性。当按分期匹配时,eoCRC的结局与loCRC相似,但由于在较年轻时出现晚期疾病的频率更高,总体死亡率更高,失去的生命年更多。迄今为止,对eoCRC的分子评估很少,与loCRC相比,发现 和 体细胞突变可能增加,而 、 和 体细胞突变减少。其他发现包括LINE-1低甲基化、微卫星不稳定性缺失(MSI-H)、染色体不稳定性(CIN)或微卫星和染色体稳定性(MACS)的存在。这些研究才刚刚出现,尚未确定定义eoCRC的特定分子特征。进一步评估eoCRC的遗传和分子差异以及环境触发因素的研究,应该能提供更清晰的认识,为有症状前风险较高的年轻个体进行针对性筛查提供依据。