Van Hollebeke Marine, Poddighe Diego, Clerckx Beatrix, Muller Jan, Hermans Greet, Gosselink Rik, Langer Daniel, Louvaris Zafeiris
Faculty of Movement and Rehabilitation Sciences, Department of Rehabilitation Sciences, Research Group for Rehabilitation in Internal Disorders, KU Leuven, Leuven, Belgium.
Department of Intensive Care Medicine, University Hospitals Leuven, Leuven, Belgium.
Front Physiol. 2022 Feb 9;13:786575. doi: 10.3389/fphys.2022.786575. eCollection 2022.
Critically ill patients who have difficulties weaning from the mechanical ventilator are prone to develop respiratory muscle weakness. Inspiratory muscle training (IMT) can improve respiratory muscle strength. Whether IMT can improve scalene and sternocleidomastoid muscle oxygenation parameters is unknown.
To compare changes in muscle oxygenation parameters of scalene and sternocleidomastoid inspiratory muscles during a standardized task between patients with weaning difficulties who received either high-intensity IMT (intervention) or sham low-intensity IMT (control).
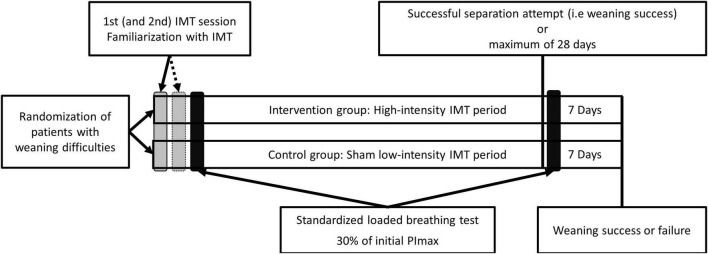
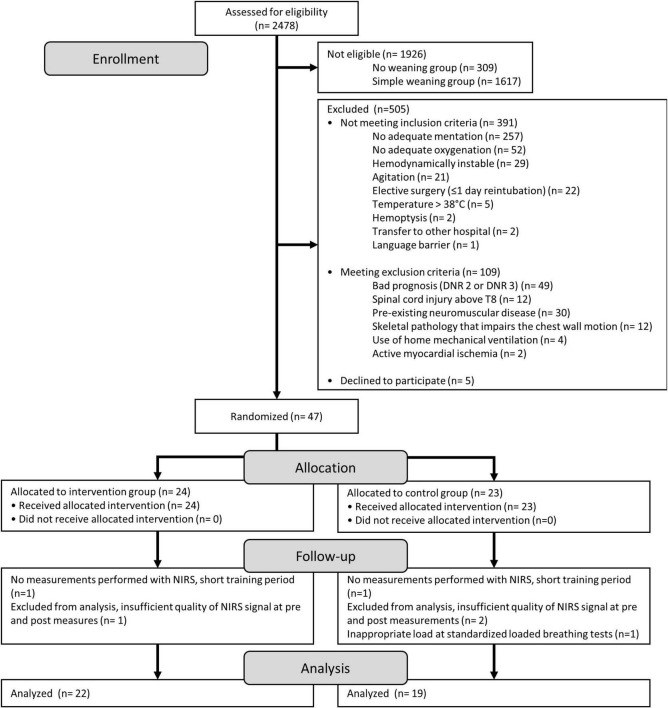
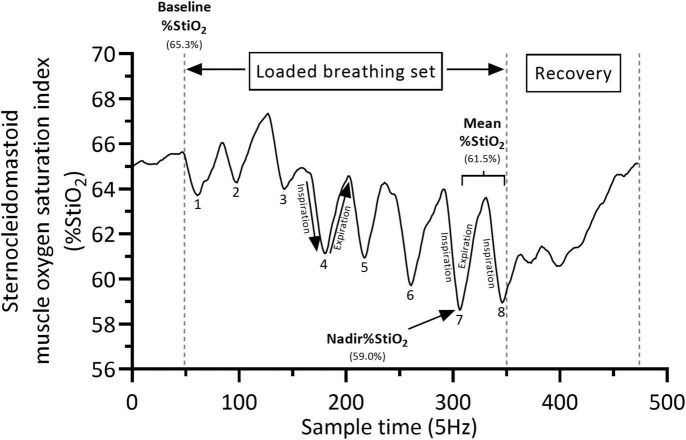
Forty-one patients performed daily IMT sessions (4 sets, 6-10 breaths) until weaning success or for 28 consecutive days. The training load was progressively adjusted in the intervention group ( = 22) to the highest tolerable load, whilst the control group ( = 19) kept training at 10% of their baseline maximal inspiratory pressure (PImax). Breathing characteristics (i.e., work and power of breathing, PoB), respiratory muscle function [i.e., PImax and forced vital capacity (FVC)] were measured during a standardized loaded breathing task against a load of 30% of baseline PImax before and after the IMT period. In addition, during the same loaded breathing task, absolute mean and nadir changes from baseline in local scalene and sternocleidomastoid muscle oxygen saturation index (Δ%StiO) (an index of oxygen extraction) and nadir Δ%StiO normalized for the PoB were measured by near-infrared spectroscopy.
At post measures, only the intervention group improved mean PoB compared to pre measures (Pre: 0.42 ± 0.33 watts, Post: 0.63 ± 0.51watts, -value < 0.01). At post measures, both groups significantly improved nadir scalene muscles StiO% normalized for the mean PoB (ΔStiO %/watt) compared to pre measurements and the improvement was not significant different between groups (-value = 0.40). However, at post measures, nadir sternocleidomastoid muscle StiO% normalized for the mean PoB (ΔStiO %/watt) was significantly greater improved in the intervention group (mean difference: +18.4, 95%CI: -1.4; 38.1) compared to the control group (mean difference: +3.7, 95%CI: -18.7; 26.0, between group -value < 0.01). Both groups significantly improved PImax (Intervention: +15 ± 13 cmHO -value < 0.01, Control: +13 ± 15 cmHO -value < 0.01). FVC only significantly improved in the intervention group (+0.33 ± 0.31 L < 0.01) report also change in control group.
This exploratory study suggests that high-intensity IMT induces greater improvements in scalene and sternocleidomastoid muscle oxygenation parameters attributed for oxygen delivery, utilization and oxygen saturation index compared to low-intensity IMT in patients with weaning difficulties.
机械通气撤机困难的重症患者容易出现呼吸肌无力。吸气肌训练(IMT)可改善呼吸肌力量。IMT是否能改善斜角肌和胸锁乳突肌的氧合参数尚不清楚。
比较接受高强度IMT(干预组)或假低强度IMT(对照组)的撤机困难患者在标准化任务期间斜角肌和胸锁乳突肌吸气肌的肌肉氧合参数变化。
41例患者每天进行IMT训练(4组,6 - 10次呼吸),直至撤机成功或持续28天。干预组(n = 22)的训练负荷逐渐调整至最高可耐受负荷,而对照组(n = 19)保持在其基线最大吸气压力(PImax)的10%进行训练。在IMT训练前后,针对相当于基线PImax 30%的负荷进行标准化负荷呼吸任务时测量呼吸特征(即呼吸功和功率,PoB)、呼吸肌功能[即PImax和用力肺活量(FVC)]。此外,在相同的负荷呼吸任务期间,通过近红外光谱测量斜角肌和胸锁乳突肌局部肌肉氧饱和度指数(Δ%StiO)(氧摄取指数)相对于基线的绝对平均值和最低点变化以及针对PoB标准化的最低点Δ%StiO。
在测量后,与测量前相比,仅干预组的平均PoB有所改善(测量前:0.42±0.33瓦,测量后:0.63±0.51瓦,P值<0.01)。在测量后,与测量前相比,两组针对平均PoB标准化的斜角肌最低点StiO%(ΔStiO %/瓦)均显著改善,且组间改善无显著差异(P值 = 0.40)。然而,在测量后,与对照组(平均差异:+3.7,95%CI: - 18.7;26.0,组间P值<0.01)相比,干预组针对平均PoB标准化的胸锁乳突肌最低点StiO%(ΔStiO %/瓦)改善更为显著(平均差异:+18.4,95%CI: - 1.4;38.1)。两组的PImax均显著改善(干预组:+15±13 cmH₂O,P值<0.01,对照组:+13±15 cmH₂O,P值<0.)。FVC仅在干预组显著改善(+0.33±0.31 L,P<0.01),对照组未报告有变化。
这项探索性研究表明,与低强度IMT相比,高强度IMT可使撤机困难患者的斜角肌和胸锁乳突肌在氧输送、利用和氧饱和度指数方面的肌肉氧合参数得到更大改善。