Prasad Rahul N, Miller Eric D, Addison Daniel, Bazan Jose G
Department of Radiation Oncology at the Arthur G. James Cancer Hospital and Richard J. Solove Research Institute, The Ohio State University Comprehensive Cancer Center, Columbus, OH, United States.
Cardio-Oncology Program, Division of Cardiology, The Ohio State University Medical Center, Columbus, OH, United States.
Front Oncol. 2022 Feb 9;12:808531. doi: 10.3389/fonc.2022.808531. eCollection 2022.
Chest radiation therapy (RT) has been associated with increased cardiac morbidity and mortality in numerous studies including the landmark Darby study published in 2013 demonstrating a linear increase in cardiac mortality with increasing mean heart radiation dose. However, the extent to which cardiotoxicity has been incorporated as an endpoint in prospective RT studies remains unknown.
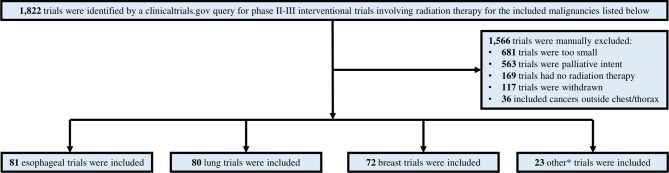
We queried clincaltrials.gov to identify phase II/III trials in lung, esophageal, lymphoma, mesothelioma, thymoma, or breast cancer from 1/1/2006-2/1/2021 enrolling greater than 100 patients wherein chest RT was delivered in at least one treatment arm. The primary endpoint was the rate of inclusion of cardiotoxicity as a specific primary or secondary endpoint in the pre- (enrollment started prior to 1/1/2014) versus post-Darby era using the Chi-square test (p<0.05 considered significant). We also analyzed clinical trial factors associated with the inclusion of cardiotoxicity as an endpoint using logistic regression analysis.
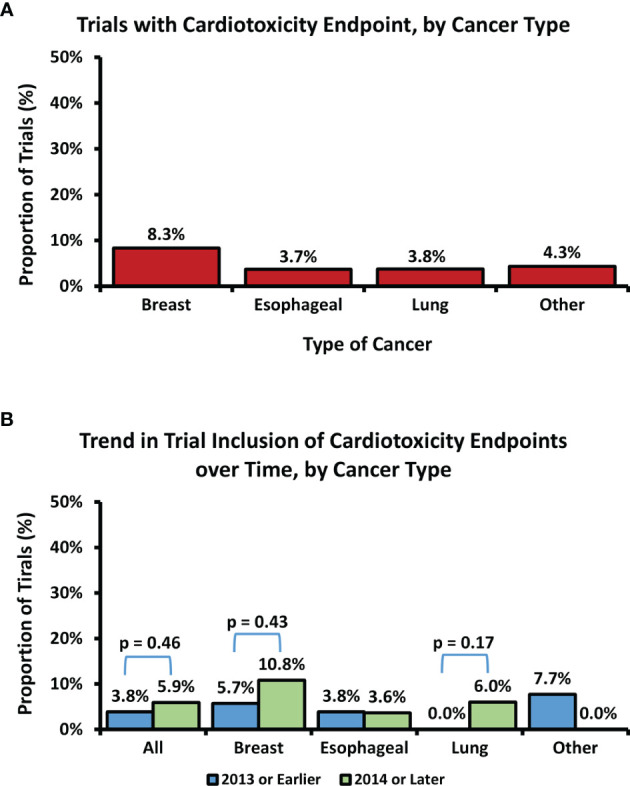
In total, 1,822 trials were identified, of which 256 merited inclusion. 32% were for esophageal, 31% lung, 28% breast, and 7% lymphoma/thymoma/mesothelioma cancers, respectively. 5% (N=13) included cardiotoxicity as an endpoint: 6 breast cancer, 3 lung cancer, 3 esophageal cancer, and 1 lymphoma study. There was no difference in the inclusion of cardiotoxicity endpoints in the pre-Darby versus post-Darby era (3.9% vs. 5.9%, P=0.46). The greatest absolute increase in inclusion of cardiotoxicity as an endpoint was seen for lung cancer (0% vs. 6%, p=0.17) and breast cancer (5.7% vs. 10.8%, p=0.43) studies, though these increases remained statistically non-significant. We found no clinical trial factors associated with the inclusion of cardiotoxicity as an endpoint.
Among prospective trials involving chest RT, cardiotoxicity remains an uncommon endpoint despite its prevalence as a primary source of toxicity following treatment. In order to better characterize cardiac toxicities, future prospective studies involving chest RT should include cardiotoxicity endpoints.
在众多研究中,胸部放射治疗(RT)与心脏发病率和死亡率增加相关,包括2013年发表的具有里程碑意义的达比研究,该研究表明心脏死亡率随平均心脏辐射剂量增加呈线性上升。然而,心脏毒性在前瞻性RT研究中作为终点指标纳入的程度仍不清楚。
我们查询了clinicaltrials.gov,以确定2006年1月1日至2021年2月1日期间纳入超过100例患者的肺癌、食管癌、淋巴瘤、间皮瘤、胸腺瘤或乳腺癌的II/III期试验,其中至少一个治疗组进行了胸部RT。主要终点是在达比时代之前(2014年1月1日之前开始入组)与之后,将心脏毒性作为特定主要或次要终点纳入的比例,采用卡方检验(p<0.05认为有统计学意义)。我们还使用逻辑回归分析了与将心脏毒性作为终点纳入相关的临床试验因素。
共识别出1822项试验,其中256项符合纳入标准。分别为食管癌试验占32%,肺癌试验占31%,乳腺癌试验占28%,淋巴瘤/胸腺瘤/间皮瘤试验占7%。5%(n = 13)将心脏毒性作为终点指标:6项乳腺癌研究、3项肺癌研究、3项食管癌研究和1项淋巴瘤研究。达比时代之前与之后将心脏毒性终点纳入的比例没有差异(3.9%对5.9%,P = 0.46)。将心脏毒性作为终点纳入的绝对增加幅度最大的是肺癌研究(0%对6%,p = 0.17)和乳腺癌研究(5.7%对10.8%,p = 0.43),尽管这些增加在统计学上仍无显著性。我们没有发现与将心脏毒性作为终点纳入相关的临床试验因素。
在涉及胸部RT的前瞻性试验中,尽管心脏毒性是治疗后主要的毒性来源,但其作为终点指标仍不常见。为了更好地描述心脏毒性,未来涉及胸部RT的前瞻性研究应纳入心脏毒性终点指标。