Greb Christopher S, Aouhab Zineb, Sisbarro Daniel, Panah Elnaz
Internal Medicine, Loyola University Medical Center, Maywood, USA.
Rheumatology, Loyola University Medical Center, Maywood, USA.
Cureus. 2022 Jan 25;14(1):e21608. doi: 10.7759/cureus.21608. eCollection 2022 Jan.
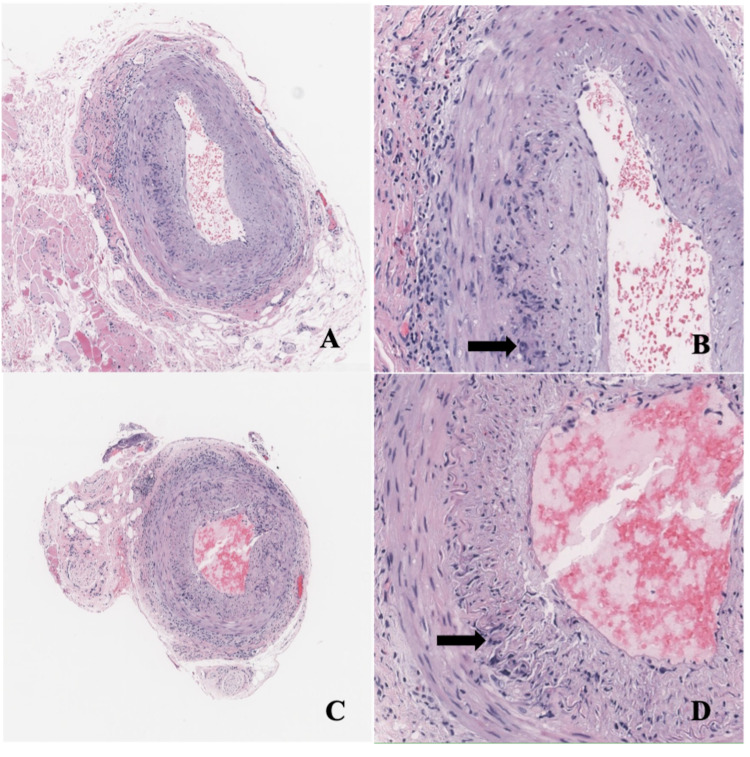
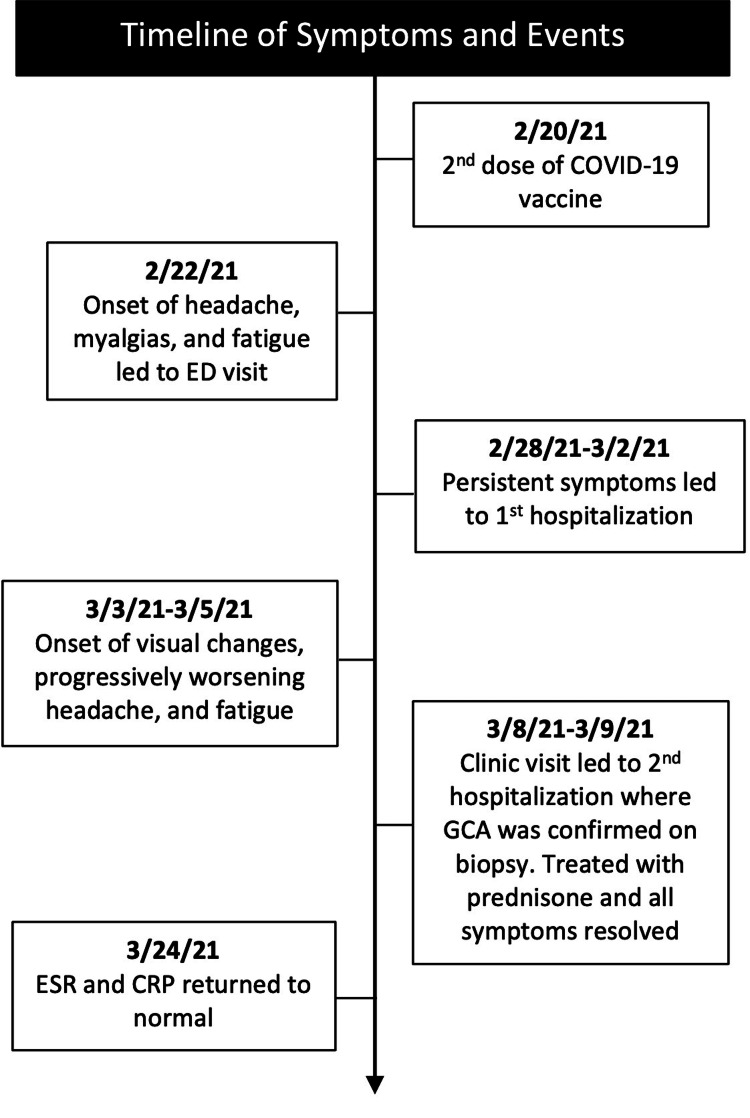
Giant cell arteritis (GCA) is a large vessel vasculitis with variable presentations, including fevers, myalgias, headache, and jaw claudication. A particularly concerning symptom is transient vision loss, which may become irreversible without prompt recognition and treatment. The pathogenesis of GCA is incompletely understood, but it seems that the innate and adaptive immune systems play a key role in vessel inflammation, remodeling, and occlusion. We present a case of a 79-year-old male who developed GCA two days after he received his second dose of a COVID-19 mRNA vaccine. He presented with headaches, fever, and myalgias. Lab workup revealed elevated inflammatory markers, with C-reactive protein (CRP) 272 mg/L (<8.1 mg/L) and erythrocyte sedimentation rate (ESR) 97 mm/hr (0-20mm/hr). Imaging of the head, with CT and MRI, was unremarkable. His headache persisted despite supportive treatment, and he developed new, transient blurred vision, which increased suspicion for GCA. He underwent bilateral temporal artery biopsies, which were consistent with GCA. His symptoms resolved quickly with oral prednisone 60mg daily, and his inflammatory markers returned to normal within a month. A review of the literature revealed several case reports of giant cell arteritis following influenza vaccination. However, no large-scale studies have demonstrated a causal relationship between GCA and immunization. Our case demonstrates the first instance of GCA following a COVID-19 mRNA vaccine. We propose that the upregulated immune response to the vaccine acted as a trigger for GCA in this patient with predisposing factors. While causation cannot be determined based on one case alone, our case demonstrates an opportunity for further research into the relationship between vasculitis and immunizations. Despite this isolated case, the proven benefits of COVID-19 mRNA vaccines significantly outweigh any theoretical risk of immune dysregulation following administration.
巨细胞动脉炎(GCA)是一种大血管血管炎,临床表现多样,包括发热、肌痛、头痛和颌部间歇性运动障碍。一个特别令人担忧的症状是短暂性视力丧失,如果不及时识别和治疗,可能会变得不可逆转。GCA的发病机制尚未完全明确,但固有免疫系统和适应性免疫系统似乎在血管炎症、重塑和闭塞过程中起关键作用。我们报告一例79岁男性病例,该患者在接种第二剂新冠病毒mRNA疫苗两天后患上GCA。他出现头痛、发热和肌痛。实验室检查显示炎症标志物升高,C反应蛋白(CRP)为272mg/L(<8.1mg/L),红细胞沉降率(ESR)为97mm/小时(0 - 20mm/小时)。头部CT和MRI成像未见明显异常。尽管进行了支持性治疗,他的头痛仍持续存在,并且出现了新的短暂性视力模糊,这增加了对GCA的怀疑。他接受了双侧颞动脉活检,结果与GCA相符。每天口服60mg泼尼松后,他的症状迅速缓解,炎症标志物在一个月内恢复正常。文献回顾显示有几例流感疫苗接种后发生巨细胞动脉炎的病例报告。然而,尚无大规模研究证明GCA与免疫接种之间存在因果关系。我们的病例是新冠病毒mRNA疫苗接种后发生GCA的首例。我们认为,对该疫苗上调的免疫反应在这个具有易感因素的患者中触发了GCA。虽然仅凭一个病例无法确定因果关系,但我们的病例为进一步研究血管炎与免疫接种之间的关系提供了机会。尽管有这一孤立病例,但新冠病毒mRNA疫苗已证实的益处显著超过接种后免疫失调的任何理论风险。