Department of Biomedical Sciences, Humanitas University, Via Rita Levi Montalcini 4, 20072 Pieve Emanuele, Milan, Italy.
IRCCS Humanitas Research Hospital, via Manzoni 56, 20089 Rozzano, Milan, Italy.
Eur Radiol. 2022 Jul;32(7):4352-4360. doi: 10.1007/s00330-022-08566-0. Epub 2022 Mar 1.
To assess clinical and cardiac magnetic resonance (CMR) imaging features of patients with peri-myocarditis following Coronavirus Disease 2019 (COVID-19) vaccination.
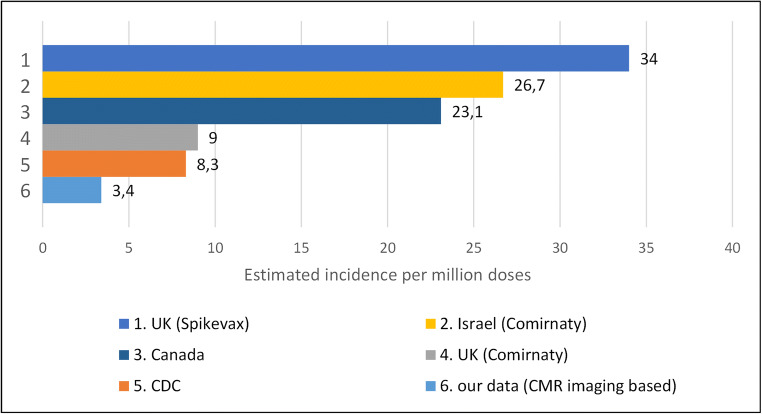
We retrospectively collected a case series of 27 patients who underwent CMR in the clinical suspect of heart inflammation following COVID-19 vaccination, from 16 large tertiary centers. Our patient's cohort was relatively young (36.6 ± 16.8 years), predominately included males (n = 25/27) with few comorbidities and covered a catchment area of approximately 8 million vaccinated patients.
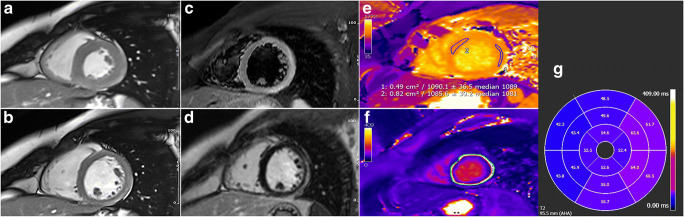
CMR revealed typical mid-subepicardial non-ischemic late gadolinium enhancement (LGE) in 23 cases and matched positively with CMR T2 criteria of myocarditis. In 7 cases, typical hallmarks of acute pericarditis were present. Short-term follow-up (median = 20 days) from presentation was uneventful for 25/27 patients and unavailable in two cases.
While establishing a causal relationship between peri-myocardial inflammation and vaccine administration can be challenging, our clinical experience suggests that CMR should be performed for diagnosis confirmation and to drive clinical decision-making and follow-up.
• Acute onset of dyspnea, palpitations, or acute and persisting chest pain after COVID-19 vaccination should raise the suspicion of possible myocarditis or pericarditis, and patients should seek immediate medical attention and treatment to help recovery and avoid complications. • In case of elevated troponin levels and/or relevant ECG changes, cardiac magnetic resonance should be considered as the best non-invasive diagnostic option to confirm the diagnosis of myocarditis or pericarditis and to drive clinical decision-making and follow-up.
评估新冠肺炎(COVID-19)疫苗接种后心肌炎患者的临床和心脏磁共振(CMR)成像特征。
我们回顾性收集了来自 16 个大型三级中心的 27 例 COVID-19 疫苗接种后临床怀疑心肌炎患者的 CMR 病例系列。我们的患者队列相对年轻(36.6±16.8 岁),主要包括男性(n=25/27),合并症较少,覆盖了约 800 万接种疫苗患者的人群。
23 例 CMR 显示典型的中下心外膜非缺血性晚期钆增强(LGE),与心肌炎的 CMR T2 标准阳性匹配。7 例存在典型的急性心包炎特征。27 例患者中有 25 例在出现症状后进行了短期随访(中位数=20 天),2 例患者的随访情况不详。
尽管确定心肌周围炎症与疫苗接种之间的因果关系具有挑战性,但我们的临床经验表明,应进行 CMR 以进行诊断确认,并为临床决策和随访提供依据。
新冠肺炎疫苗接种后出现呼吸困难、心悸或急性和持续胸痛应高度怀疑可能发生心肌炎或心包炎,患者应立即就医并接受治疗,以帮助康复并避免并发症。
在肌钙蛋白水平升高和/或相关心电图变化的情况下,应考虑心脏磁共振作为确认心肌炎或心包炎诊断以及为临床决策和随访提供依据的最佳非侵入性诊断选择。