Staehler Michael, Schuler Tina, Spek Annabel, Rodler Severin, Tamalunas Alexander, Fürweger Christoph, Muacevic Alexander
Urology, University Hospital, Ludwig Maximilians University Munich, Munich, DEU.
Medical Physics, European CyberKnife Center, Munich, DEU.
Cureus. 2022 Jan 26;14(1):e21623. doi: 10.7759/cureus.21623. eCollection 2022 Jan.
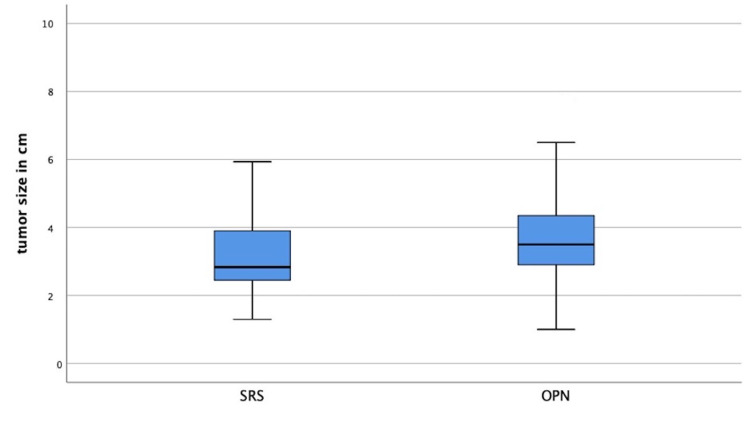
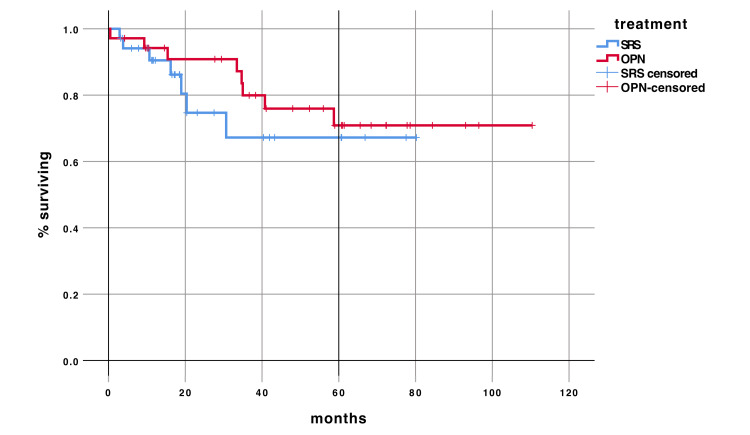
Introduction High-dose local stereotactic robotic radiosurgery (RRS) is a non-invasive alternative to surgery in renal masses and selected patients. We have, so far, limited its use to the elderly and patients at high risk from surgery. In this study, we matched patients with renal tumors who were treated with single fraction RRS to patients who underwent open partial nephrectomy (OPN). Methods Between January 2009 and December 2017, we included 571 consecutive patients undergoing OPN and 99 patients who underwent RRS in this retrospective analysis. Patients had to have a follow-up of at least six months and we were able to match 35 with a propensity score. Matching criteria were Eastern Cooperative Oncology Group (ECOG) status, age, clinical tumor, nodes, and metastases (TNM), and tumor diameter. Tumor response, renal function, survival, and adverse events were evaluated every three months until progression or death. Results Median age was 65 years for RRS (range 58-75) and 71 (range 56-76) for OPN (p=0.131). Median diameter of renal tumors was 2.8 cm (range 2.4-3.9) for RRS and 3.5 cm (2.8-4.5) for OPN, p=0.104. Median follow-up was 28.1 months (range 6.0-78.3 months). Local tumor control nine months after RRS and OPN was 98% (95% CI: 89-99%). Renal function remained stable with a median creatinine clearance (Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI)) at baseline of 76.8mlmin/1.73m (range 25.3-126.3) and 70.3ml/min/1.73m (range 18.6-127.3) at follow-up (p=0.89). Median overall survival was not reached. No difference in overall survival (OS) was seen in RRS compared to OPN (p=0.459). Conclusions Single fraction RRS is an alternative to OPN in patients unfit for surgery. Oncological and functional results are comparable to those of OPN. Further studies are needed to determine long-term results and limits of RRS in this setting and in younger patients.
引言 高剂量局部立体定向机器人放射外科手术(RRS)是肾肿瘤及特定患者手术的一种非侵入性替代方法。到目前为止,我们将其应用局限于老年患者及手术高风险患者。在本研究中,我们将接受单次分割RRS治疗的肾肿瘤患者与接受开放性部分肾切除术(OPN)的患者进行了匹配。
方法 在2009年1月至2017年12月期间,我们纳入了571例连续接受OPN的患者和99例接受RRS的患者进行这项回顾性分析。患者必须至少随访6个月,我们能够通过倾向评分匹配35例患者。匹配标准为东部肿瘤协作组(ECOG)状态、年龄、临床肿瘤、淋巴结和转移情况(TNM)以及肿瘤直径。每三个月评估一次肿瘤反应、肾功能、生存率和不良事件,直至疾病进展或死亡。
结果 RRS组患者的中位年龄为65岁(范围58 - 75岁),OPN组为71岁(范围56 - 76岁)(p = 0.131)。RRS组肾肿瘤的中位直径为2.8 cm(范围2.4 - 3.9 cm),OPN组为3.5 cm(2.8 - 4.5 cm),p = 0.104。中位随访时间为28.1个月(范围6.0 - 78.3个月)。RRS和OPN术后9个月的局部肿瘤控制率为98%(95%CI:89 - 99%)。肾功能保持稳定,基线时肌酐清除率(慢性肾脏病流行病学协作组(CKD - EPI))中位数为76.8ml/min/1.73m²(范围25.3 - 126.3),随访时为70.3ml/min/1.73m²(范围18.6 - 127.3)(p = 0.89)。总生存期未达到中位数。RRS组与OPN组的总生存期(OS)无差异(p = 0.459)。
结论 单次分割RRS是不适合手术患者的OPN替代方法。肿瘤学和功能结果与OPN相当。需要进一步研究以确定RRS在此情况下以及年轻患者中的长期结果和局限性。