Department of Internal Medicine, Seoul National University Bundang Hospital, 300 Gumi-dong, Bundang-gu, Seongnam, Gyeonggi-do, 463-707, South Korea.
Department of Internal Medicine and Liver Research Institute, Seoul National University College of Medicine, Seoul, South Korea.
BMC Gastroenterol. 2022 Mar 2;22(1):91. doi: 10.1186/s12876-022-02177-1.
To evaluate whether the risk of metachronous high-risk colorectal neoplasm (HR-CRN) differs according to the indication for surveillance colonoscopy.
Patients who underwent polypectomy or endoscopic resection of colorectal neoplasms were enrolled and classified into three groups according to the indication for surveillance colonoscopy: advanced colorectal neoplasm (ACRN: adenoma ≥ 10 mm, adenoma with high-degree dysplasia and/or villous component), advanced serrated polyps (ASP: hyperplastic polyp or sessile serrated lesion ≥ 10 mm, traditional serrated polyp), and high-risk polyps (HRP: 3 or more adenomas or serrated polyps). The primary outcome was the development of metachronous HR-CRN, defined as ACRN, ASP, or HRP at the first follow-up colonoscopy.
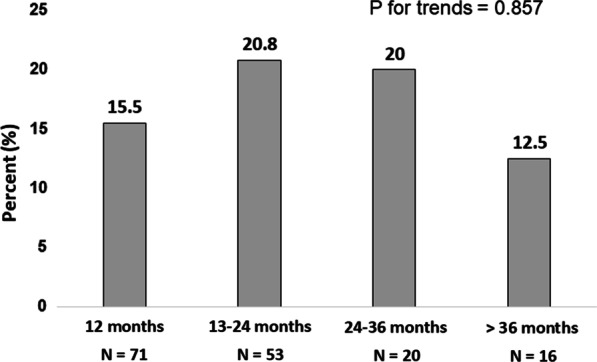
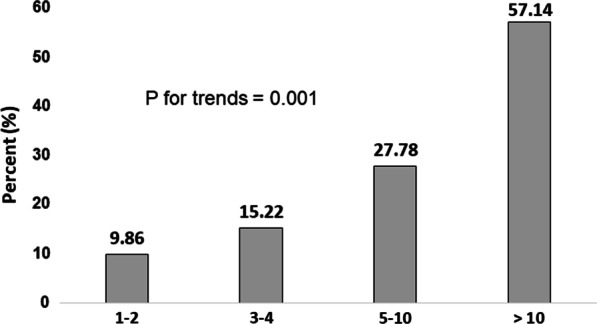
In total, 367 patients were enrolled (ACRN group: N = 264; ASP group: N = 33; HRP group: N = 70). Among the 160 patients who underwent follow-up colonoscopy, 28 (18%) had HR-CRN. In univariable analysis, indication for surveillance colonoscopy was not found to be associated with the development of metachronous HR-CRN. Instead, the total polyp number at index colonoscopy showed a positive association with the risk of metachronous HR-CRN in trend analysis (p = 0.001). In multivariable analysis, the presence of 5 or more polyps at index colonoscopy was found to be associated with the risk of metachronous HR-CRN (OR, 2.575, p = 0.049) after adjusting for risk factors, such as obesity, diabetes, and smoking.
The risk of metachronous HR-CRN did not differ according to the main indications for surveillance colonoscopy. The presence of 5 or more polyps at index colonoscopy was the only risk factor for metachronous HR-CRN.
评估基于结肠镜监测适应证的不同,结直肠腺瘤患者发生异时性高危结直肠肿瘤(HR-CRN)的风险是否存在差异。
纳入接受结直肠肿瘤息肉切除术或内镜下切除术的患者,并根据结肠镜监测的适应证将其分为三组:进展期结直肠肿瘤(ACRN:腺瘤≥10mm,高级别异型增生和/或绒毛成分的腺瘤)、进展期锯齿状息肉(ASP:增生性息肉或无蒂锯齿状病变≥10mm,传统锯齿状息肉)和高危息肉(HRP:3 个或更多腺瘤或锯齿状息肉)。主要结局是在首次随访结肠镜检查时发生异时性 HR-CRN,定义为 ACRN、ASP 或 HRP。
共纳入 367 例患者(ACRN 组:N=264;ASP 组:N=33;HRP 组:N=70)。在接受随访结肠镜检查的 160 例患者中,28 例(18%)发生 HR-CRN。单变量分析显示,结肠镜监测的适应证与异时性 HR-CRN 的发生无关。相反,在趋势分析中,索引结肠镜检查时的总息肉数量与异时性 HR-CRN 的风险呈正相关(p=0.001)。多变量分析显示,在调整肥胖、糖尿病和吸烟等危险因素后,索引结肠镜检查时存在 5 个或更多息肉与异时性 HR-CRN 的风险相关(OR,2.575,p=0.049)。
基于结肠镜监测适应证的不同,结直肠腺瘤患者发生异时性 HR-CRN 的风险无差异。索引结肠镜检查时存在 5 个或更多息肉是异时性 HR-CRN 的唯一危险因素。