Division of Spine Surgery, Department of Orthopedic Surgery, Affiliated Drum Tower Hospital, Medical School of Nanjing University, Zhongshan Road 321, Nanjing, 210008, China.
Medical School of Nanjing University, Nanjing, China.
BMC Musculoskelet Disord. 2022 Mar 2;23(1):194. doi: 10.1186/s12891-022-05140-z.
The study aimed to evaluate the influence of thoracolumbar kyphosis secondary to ankylosing spondylitis (AS) on parameters of S2AI trajectory and to compare the ideal S2AI trajectory with those of the non-deformity patients with AS, sagittal deformity patients without AS, and the normal population reported in literatures.
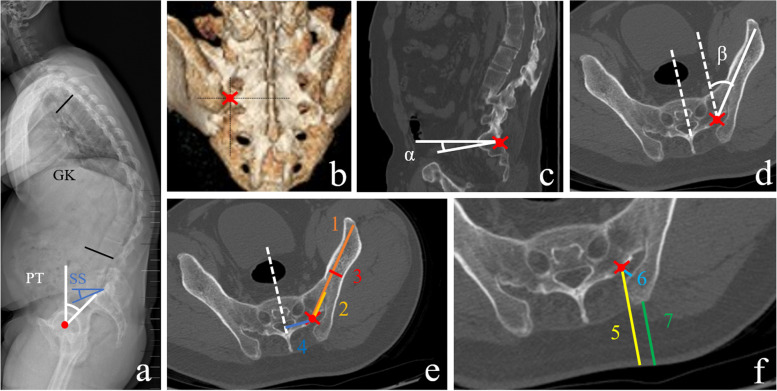
Sagittal parameters including global kyphosis (GK), pelvic tilt (PT) and sacral slope (SS) were measured. Besides, according to the simulated ideal S2AI trajectory on the CT images, trajectory parameters were measured including Sag angle, Tsv angle, Max-length, Sacral distance and Iliac width. Starting-point parameters were also measured including PSIS distance, Skin distance, Iliac wing and S2 midline.
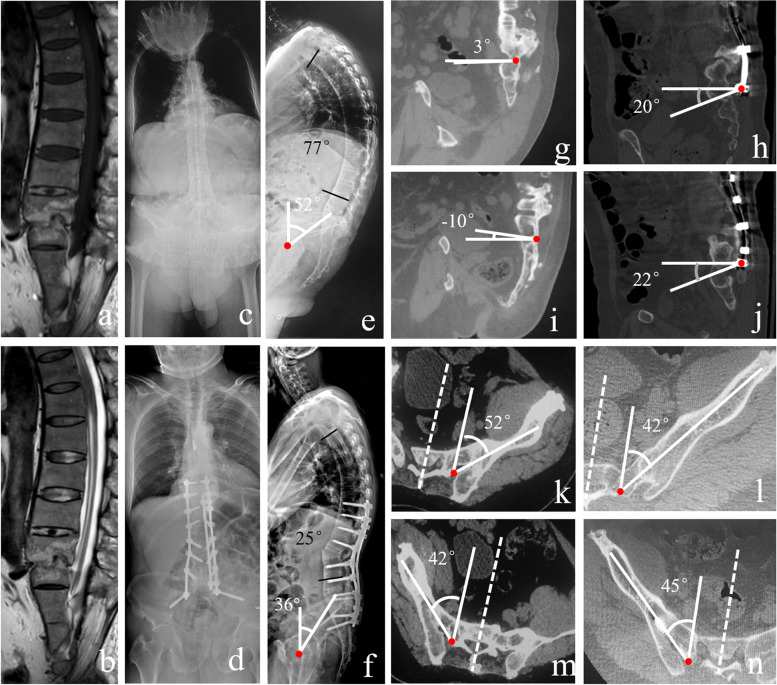
Ninety-four AS-related thoracolumbar kyphosis patients were included. After adjusting the age and gender, twenty non-deformity patients with AS and 20 sagittal deformity patients without AS were selected to compare with patients with AS-related thoracolumbar kyphosis, respectively. Sag angle in deformity patients with AS was smaller than other two groups (P < 0.001). No difference was found in Tsv angle and Sacral distance between AS patients with and without deformity. However, these two parameters were shown significant differences between deformity patients with AS and without AS. In deformity patients with AS, no significant differences were found in all parameters between genders Furthermore, there were strong correlations between PT and the bilateral Sag angle (P < 0.001).
The thoracolumbar kyphosis secondary to AS affects the Sag angle of the ideal S2AI trajectory which was approximately 20° smaller than that in non-deformity patients with AS, sagittal deformity patients without AS, and the normal population. Additionally, the Tsv angle and the Sacral distance in AS patients with thoracolumbar kyphosis were about 10° and 10 mm larger than those in sagittal deformity patients without AS, and the normal population reported in literatures.
本研究旨在评估强直性脊柱炎(AS)继发胸腰椎后凸对 S2AI 轨迹参数的影响,并比较理想 S2AI 轨迹与非畸形 AS 患者、无 AS 矢状位畸形患者以及文献报道的正常人群的差异。
测量矢状面参数,包括全局后凸角(GK)、骨盆倾斜角(PT)和骶骨倾斜角(SS)。此外,根据 CT 图像上模拟的理想 S2AI 轨迹,测量轨迹参数,包括 Sag 角、Tsv 角、最大长度、骶骨距离和髂骨宽度。还测量了起始点参数,包括 PSIS 距离、皮肤距离、髂嵴和 S2 中线。
共纳入 94 例 AS 相关胸腰椎后凸患者。调整年龄和性别后,分别选择 20 例非畸形 AS 患者和 20 例无 AS 矢状位畸形患者与 AS 相关胸腰椎后凸患者进行比较。AS 畸形患者的 Sag 角明显小于其他两组(P<0.001)。AS 患者中,畸形与非畸形组间 Tsv 角和骶骨距离无差异。然而,这两个参数在 AS 畸形患者与无畸形患者之间存在显著差异。在 AS 畸形患者中,两性间各参数均无显著差异。此外,PT 与双侧 Sag 角之间存在很强的相关性(P<0.001)。
AS 继发胸腰椎后凸会影响理想 S2AI 轨迹的 Sag 角,使其比非畸形 AS 患者、无 AS 矢状位畸形患者和文献报道的正常人群小约 20°。此外,AS 合并胸腰椎后凸患者的 Tsv 角和骶骨距离比无 AS 矢状位畸形患者和文献报道的正常人群大约 10°和 10mm。