Shenzhen Key Laboratory of Reproductive Immunology for Peri-Implantation, Shenzhen Zhongshan Institute for Reproduction and Genetics, Fertility Center, Shenzhen Zhongshan Urology Hospital, Shenzhen, PR China.
Reproductive Medical Center, Renmin Hospital of Wuhan University & Hubei Clinic Research Center for Assisted Reproductive Technology and Embryonic Development, Wuhan, PR China.
BMC Pregnancy Childbirth. 2022 Mar 2;22(1):171. doi: 10.1186/s12884-022-04518-0.
The current study was undertaken to investigate the relationship between antimüllerian hormone (AMH) and polycystic ovarian syndrome (PCOS) phenotypes and to determine whether AMH is associated with pregnancy outcomes in infertile women undergoing their first in vitro fertilization (IVF) treatment.
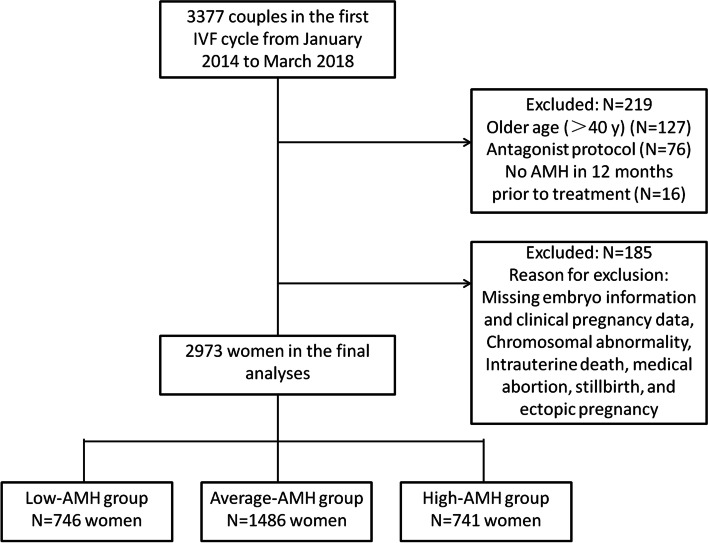
We performed a retrospective cohort study of 2973 infertile women, including 418 women with PCOS undergoing their first IVF treatment at a private fertility center from January 2014 to March 2018. Women were stratified into three groups using cutoffs defined by the 25 and 75 percentiles of the serum AMH level: 746 women had AMH ≤ 2.25 ng/mL; 1486 women had AMH between 2.25 to 5.71 ng/mL; and 741 women had AMH > 5.71 ng/mL. Endocrine characteristics, PCOS phenotypes, stimulation outcomes, pregnancy outcomes were compared among these groups. When there were any statistical differences (P < 0.05) among the three groups, Bonferroni test was performed as post-hoc tests to determine where the statistical differences existed. To assess the relationships between AMH and pregnancy outcomes in total patients and PCOS patients, logistic regression analysis, adjusted for potential confounding covariates, were performed.
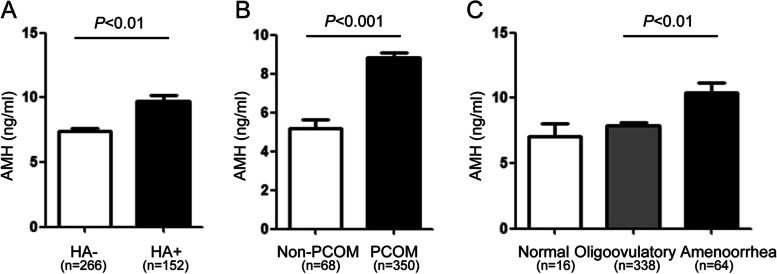
Women with high AMH had greater prevalence of hyperandrogenism (HA), polycystic ovarian morphology (PCOM) and amenorrhea than women with low or average AMH. The clinical pregnancy rate were significantly higher in the high-AMH group compared with low- and average-AMH groups (69.9% vs. 58.8% and 64.7% respectively; P < 0.001). The live birth rate was significantly lower in women with AMH ≤ 2.25 ng/mL compared with average- and high-AMH groups (47.6% vs. 55.2 and 59.5% respectively; P < 0.001). However, after controlling for maternal age, oocyte yield, as well as other confounders, AMH was no longer associated with a higher live birth rate (aOR 1.037, 95% CI 0.853-1.261, P = 0.717; aOR 1.099, 95% CI 0.858-1.408, P = 0.455, respectively) and clinical pregnancy rate (aOR 1.064, 95% CI 0.834-1.359, P = 0.617; aOR 1.181, 95% CI 0.875-1.595, P = 0.276, respectively). Moreover, pregnancy outcomes did not differ in PCOS women according to AMH quartiles.
Increased AMH levels associated with PCOS severity and greater ovarian stimulation. However, AMH was not associated with clinical pregnancy rate and live birth rate after controlling for other confounders in women undergoing IVF. Thus, AMH should not be used to alter clinical decisions and exclude patients based on a low or even undetectable AMH value.
本研究旨在探讨抗缪勒管激素(AMH)与多囊卵巢综合征(PCOS)表型的关系,并确定 AMH 是否与接受首次体外受精(IVF)治疗的不孕妇女的妊娠结局相关。
我们对 2973 名不孕妇女进行了回顾性队列研究,其中包括 2014 年 1 月至 2018 年 3 月在一家私人生育中心接受首次 IVF 治疗的 418 名 PCOS 妇女。妇女按血清 AMH 水平的 25 和 75 百分位定义的截点分为三组:746 名妇女的 AMH≤2.25ng/mL;1486 名妇女的 AMH 在 2.25 至 5.71ng/mL 之间;741 名妇女的 AMH>5.71ng/mL。比较这些组之间的内分泌特征、PCOS 表型、刺激结局和妊娠结局。当三组之间存在任何统计学差异(P<0.05)时,采用 Bonferroni 检验作为事后检验,以确定统计学差异存在的位置。为了评估 AMH 与总患者和 PCOS 患者妊娠结局之间的关系,进行了 logistic 回归分析,并调整了潜在的混杂协变量。
高 AMH 组妇女的高雄激素血症(HA)、多囊卵巢形态(PCOM)和闭经发生率高于低 AMH 和中 AMH 组。与低 AMH 和中 AMH 组相比,高 AMH 组的临床妊娠率显著更高(分别为 69.9%、58.8%和 64.7%;P<0.001)。与中 AMH 和高 AMH 组相比,AMH≤2.25ng/mL 的妇女的活产率显著降低(分别为 47.6%、55.2%和 59.5%;P<0.001)。然而,在校正了母亲年龄、卵母细胞产量以及其他混杂因素后,AMH 与更高的活产率(比值比 1.037,95%置信区间 0.853-1.261,P=0.717;比值比 1.099,95%置信区间 0.858-1.408,P=0.455)和临床妊娠率(比值比 1.064,95%置信区间 0.834-1.359,P=0.617;比值比 1.181,95%置信区间 0.875-1.595,P=0.276)不再相关。此外,根据 AMH 四分位数,PCOS 妇女的妊娠结局没有差异。
较高的 AMH 水平与 PCOS 的严重程度和更大的卵巢刺激相关。然而,在校正了其他混杂因素后,AMH 与接受 IVF 治疗的妇女的临床妊娠率和活产率无关。因此,AMH 不应被用于改变临床决策,并排除基于低或甚至无法检测到的 AMH 值的患者。