Han Hongxing, Wang Yu, Wang Hao, Sun Hongyang, Wang Xianjun, Gong Jian, Huo Xiaochuan, Zhu Qiyi, Che Fengyuan
Department of Neurology, Linyi People's Hospital, Linyi, China.
Department of Interventional Neuroradiology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China.
Front Neurol. 2022 Feb 14;12:801024. doi: 10.3389/fneur.2021.801024. eCollection 2021.
To date, no consensus still exists on the anesthesia strategy of endovascular treatment (EVT) for acute ischemic stroke (AIS) due to large vessel occlusion (LVO). We aimed to compare the 90-day outcomes, puncture-to-recanalization time (PRT), successful recanalization rate, and symptomatic intracranial hemorrhage (sICH) of patients undergoing general anesthesia (GA) or local anesthesia (LA) ± conscious sedation (CS) during the procedure.
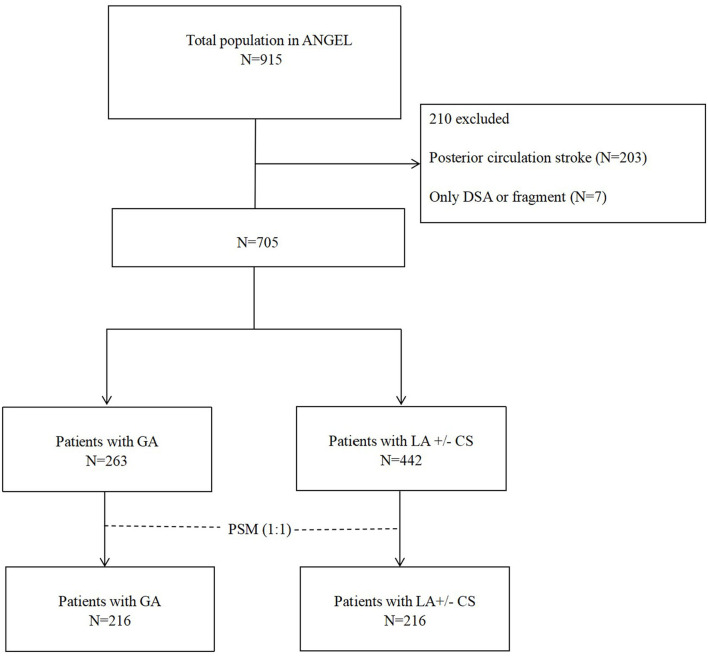
We selected patients from the Acute Ischemic Stroke Cooperation Group of Endovascular Treatment (ANGEL) registry and divided them into the GA group and the LA ± CS group. The two groups underwent 1:1 matching under propensity score matching (PSM) analysis. Then, we compared the primary outcome including the 90-day modified Rankin Scale (mRS) 0-2, secondary outcome including the 90-day mRS, the 90-day mRS 0-1, the 90-day mRS 0-3, PRT, and successful recanalization rate as well as the safety outcome including sICH, any ICH, and 90-day mRS 6.
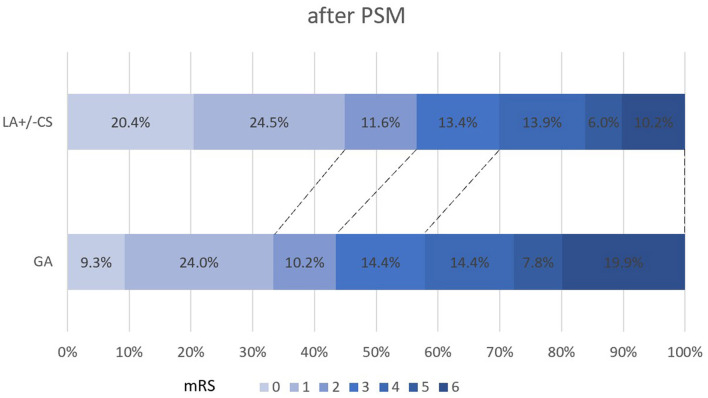
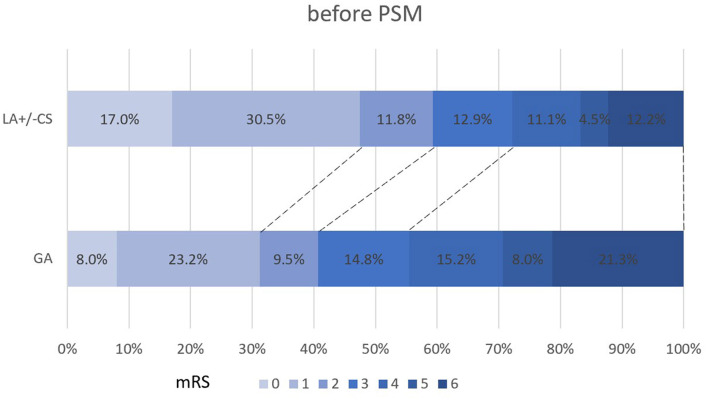
Among the 705 enrolled patients, 263 patients underwent GA and 442 patients underwent LA ± CS. After 1:1 PSM according to the baseline characteristics, each group has 216 patients. Patients with GA had the higher median 90-day mRS [3 (1-5) vs. 2 (1-4), < 0.001], the lower 90-day mRS 0-2 rate (43.5 vs. 56.5%, = 0.007), higher mortality (19.9 vs.10.2%, = 0.005), and longer PRT [92 (60-140) vs. 70 (45-103) min, < 0.001]. There were no differences in sICH and successful recanalization rate between both the groups.
In the real-world setting, LA ± CS might provide more outcomes benefits than GA in patients with AIS-LVO during the procedure.
迄今为止,对于因大血管闭塞(LVO)导致的急性缺血性卒中(AIS)进行血管内治疗(EVT)的麻醉策略仍未达成共识。我们旨在比较在手术过程中接受全身麻醉(GA)或局部麻醉(LA)±清醒镇静(CS)的患者的90天预后、穿刺至再通时间(PRT)、成功再通率和症状性颅内出血(sICH)情况。
我们从血管内治疗急性缺血性卒中合作组(ANGEL)登记处选取患者,并将他们分为GA组和LA±CS组。在倾向评分匹配(PSM)分析下,两组进行1:1匹配。然后,我们比较主要结局,包括90天改良Rankin量表(mRS)评分为0 - 2,次要结局,包括90天mRS评分、90天mRS评分为0 - 1、90天mRS评分为0 - 3、PRT和成功再通率,以及安全性结局,包括sICH、任何颅内出血和90天mRS评分为6。
在705名登记患者中,263名患者接受GA,442名患者接受LA±CS。根据基线特征进行1:1 PSM后,每组有216名患者。接受GA的患者90天mRS中位数更高[3(1 - 5)对2(1 - 4),P < 0.001],90天mRS为0 - 2的比例更低(43.5%对56.5%,P = 0.007),死亡率更高(19.9%对10.2%,P = 0.005),PRT更长[92(60 - 140)分钟对70(45 - 103)分钟,P < 0.001]。两组之间的sICH和成功再通率没有差异。
在现实环境中,对于AIS - LVO患者,在手术过程中LA±CS可能比GA带来更多的预后益处。