Campbell A J, Dotel R, Braddick M, Britton P N, Eisen D P, Francis J R, Lynar S, McMullan B, Meagher N, Nelson J, O'Sullivan M V N, Price D J, Robinson J O, Whelan A, Tong S Y C, Bowen A C, Davis J S
Department of Infectious Diseases, Perth Children's Hospital, Perth, Australia.
Wesfarmers Centre of Vaccines and Infectious Diseases, Telethon Kids Institute, Perth, Australia.
JAC Antimicrob Resist. 2022 Feb 17;4(1):dlac014. doi: 10.1093/jacamr/dlac014. eCollection 2022 Mar.
Combination antibiotic therapy with an antitoxin agent, such as clindamycin, is included in some guidelines for severe, toxin-mediated infections. The evidence to support this practice is currently limited to animal and observational human case-series data, with no previous randomized controlled trials (RCTs).
This pilot RCT aimed to determine the feasibility of conducting a clinical trial to examine if adjunctive clindamycin with standard therapy has greater efficacy than standard therapy alone for infections.
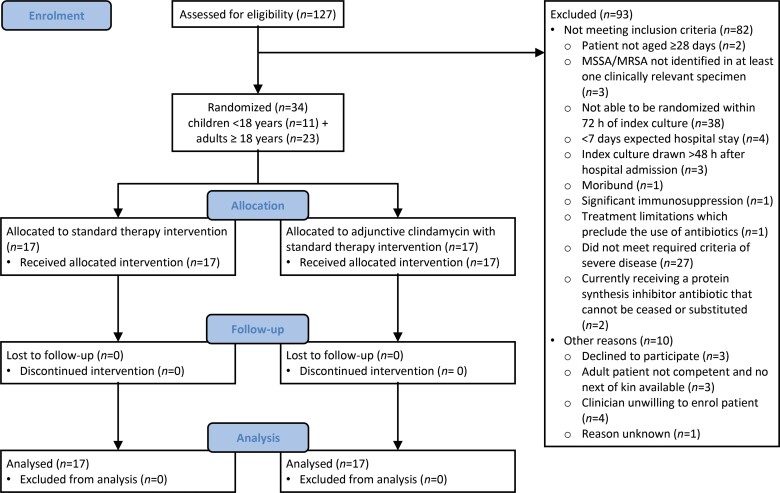
We performed an investigator-initiated, open-label, multicentre, pilot RCT (ACTRN12617001416381p) in adults and children with severe infections, randomized to standard antibiotic therapy with or without clindamycin for 7 days.
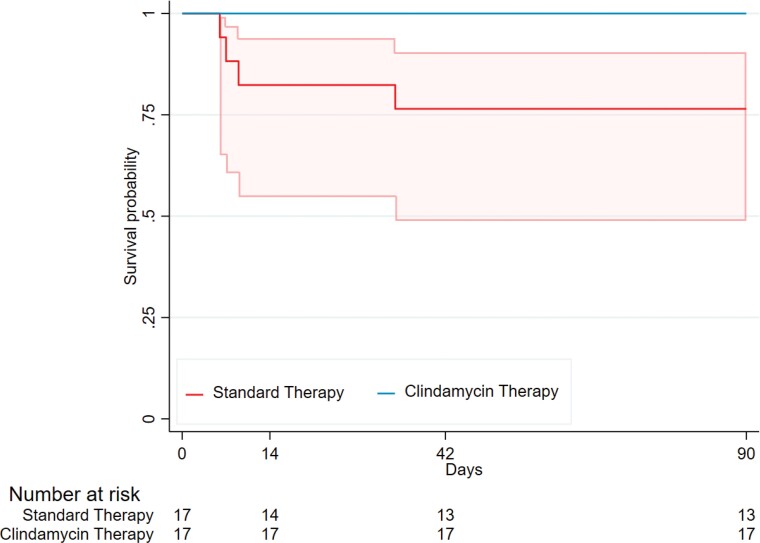
Over 28 months, across nine sites, 127 individuals were screened and 34 randomized, including 11 children (32%). The primary outcome-number of days alive and free of systemic inflammatory response syndrome ≤14 days-was similar between groups: clindamycin (3 days [IQR 1-6]) versus standard therapy (4 days [IQR 0-8]). The 90 day mortality was 0% (0/17) in the clindamycin group versus 24% (4/17) in the standard therapy group. Secondary outcomes-microbiological relapse, treatment failure or diarrhoea-were similar between groups.
As the first clinical trial assessing adjunctive clindamycin for infections, this study indicates feasibility and that adults and children can be incorporated into one trial using harmonized endpoints, and there were no safety concerns. The CASSETTE trial will inform the definitive Network Adaptive Platform (SNAP) trial, which includes an adjunctive clindamycin domain and participants with non-severe disease.
在一些针对严重的、毒素介导的感染的指南中,包含了联合使用抗生素与抗毒素药物(如克林霉素)的治疗方法。目前支持这种治疗方法的证据仅限于动物实验和观察性人类病例系列数据,此前尚无随机对照试验(RCT)。
这项初步随机对照试验旨在确定开展一项临床试验的可行性,以检验在感染治疗中,标准治疗联合克林霉素是否比单纯标准治疗更有效。
我们开展了一项由研究者发起的、开放标签、多中心的初步随机对照试验(ACTRN12617001416381p),纳入患有严重感染的成人和儿童,随机分为接受7天标准抗生素治疗加或不加克林霉素的两组。
在28个月内,涉及9个地点,共筛查了127人,34人被随机分组,其中包括11名儿童(32%)。主要结局指标——存活且无全身炎症反应综合征的天数≤14天——两组相似:克林霉素组为3天(四分位间距1 - 6),标准治疗组为4天(四分位间距0 - 8)。克林霉素组90天死亡率为0%(0/17),标准治疗组为24%(4/17)。次要结局指标——微生物复发、治疗失败或腹泻——两组相似。
作为第一项评估克林霉素辅助治疗感染的临床试验,本研究表明了其可行性,且成人和儿童可纳入同一试验并使用统一的终点指标,并且不存在安全性问题。“CASSETTE试验”将为确定性的“网络适应性平台(SNAP)试验”提供信息,后者包括一个克林霉素辅助治疗领域以及患有非严重疾病的参与者。