From the Rush Alzheimer's Disease Center (A.R.Z., Y.L., J.A.S., D.A.B., A.S.B.), Department of Psychiatry and Behavioral Sciences (A.R.Z.), Department of Neurological Sciences (Y.L., J.A.S., D.A.B., A.S.B.), and Department of Pathology (J.A.S.), Rush University Medical Center, Chicago, IL; Biological Sciences Division (V.P.), Pacific Northwest National Laboratory, Richland, WA; and Center for Translational & Computational Neuroimmunology (P.L.D.J., H.-U.K.), Department of Neurology, Columbia University Medical Center, New York, NY.
Neurology. 2022 Mar 29;98(13):e1304-e1314. doi: 10.1212/WNL.0000000000200017. Epub 2022 Mar 3.
Cognitive resilience is a well-recognized concept, but knowledge gaps about its underlying mechanisms have made it difficult to develop instruments that identify older adults with high or low resilience. We tested whether aggregating cortical peptides associated with cognitive resilience into an index can identify adults with higher or lower cognitive resilience.
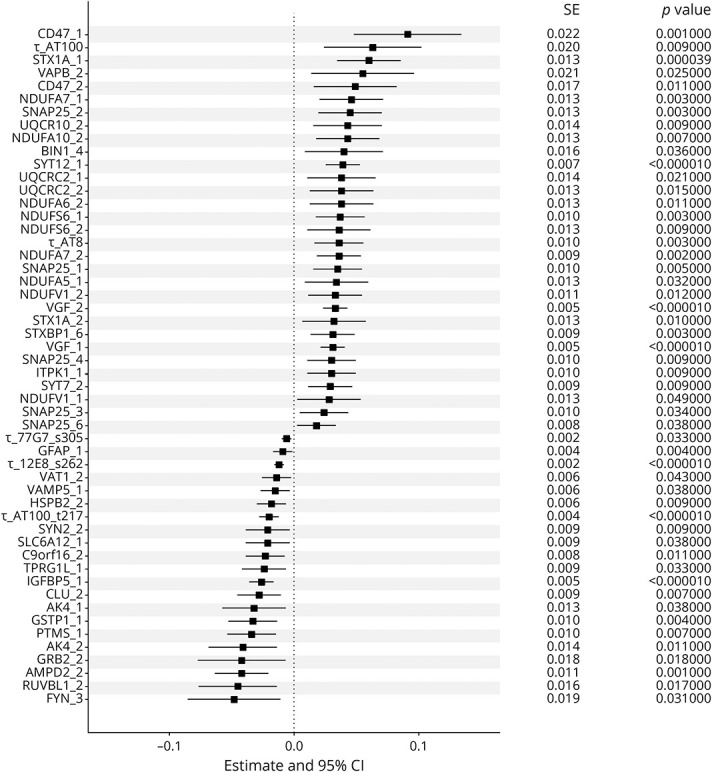
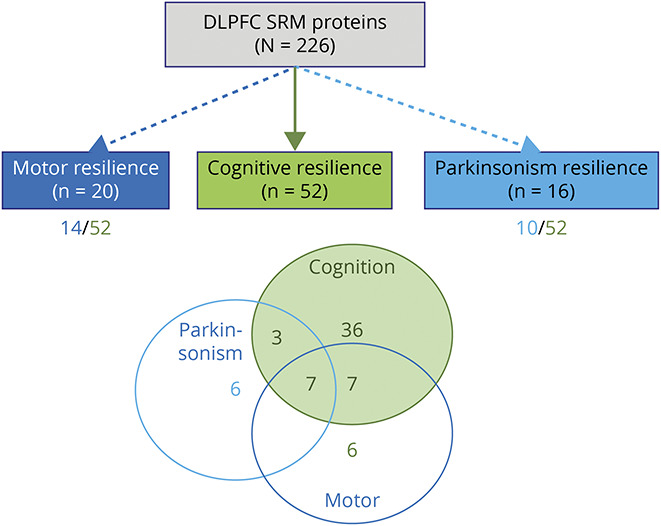
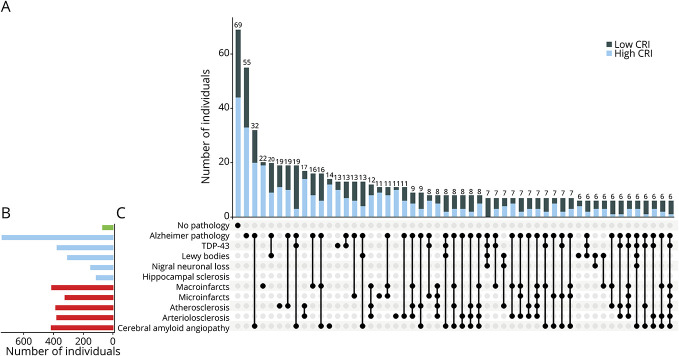
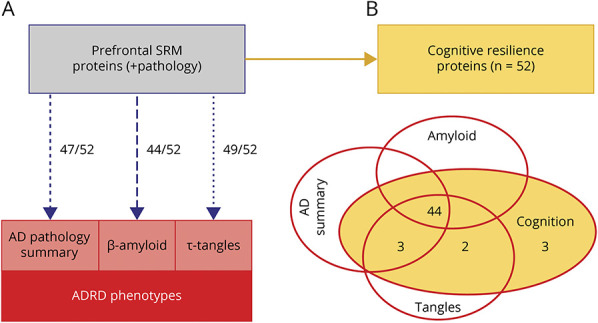
We used data from 1,192 older decedents, including annual clinical testing, indices of 10 Alzheimer disease (AD) and related dementia (ADRD) pathologies, and 226 proteotypic peptides measured in the dorsal lateral prefrontal cortex. We used linear mixed-effects models to identify peptides that were related to cognitive resilience (i.e., cognitive decline not explained by ADRD pathologies [false discovery rate <0.05]). We aggregated the expression levels of these resilience peptides into a person-specific cognitive resilience index and examined its association with AD clinical and pathologic phenotypes.
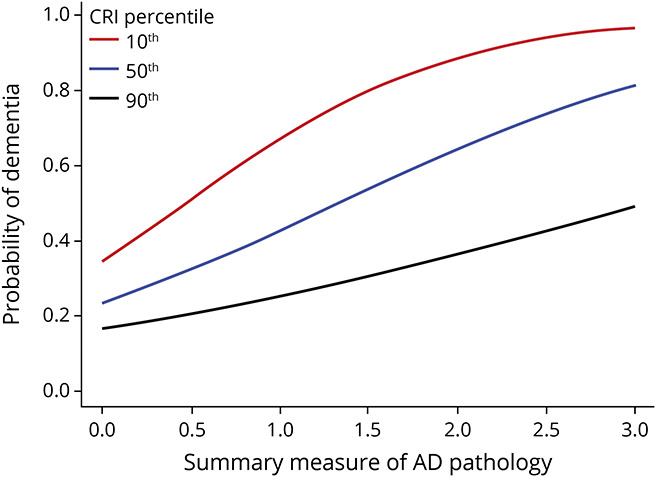
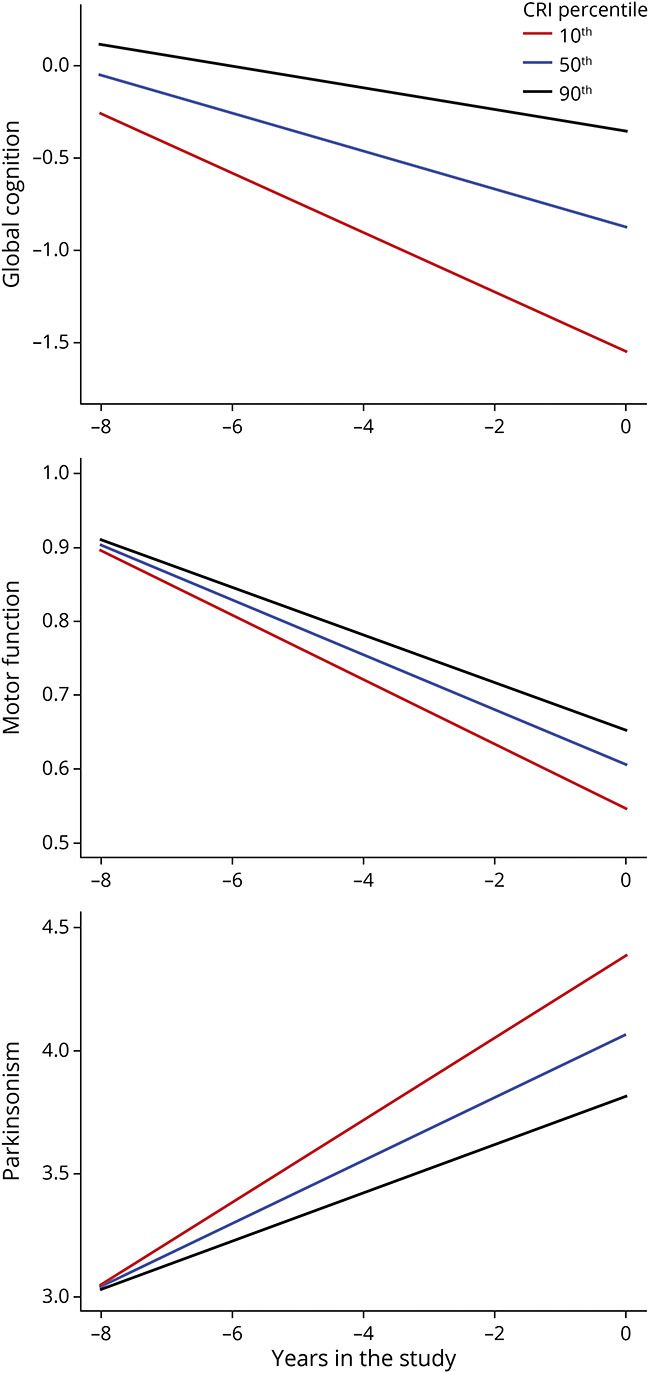
We constructed a resilience index from 52 of 226 peptides related to cognitive resilience. A higher index was associated with slower cognitive decline (estimate 0.05, SE 0.003, < 0.001) and slower motor decline (estimate 0.005, SE 0.001, < 0.001). Most resilience peptides (70%) were specific to cognitive decline, but 30% also provided resilience for motor decline. A higher index was also related to a lower burden of AD pathologies (odds ratio [OR] 0.41, SE 0.01, < 0.001) and modified the association of AD pathology with cognition in that a higher index modified the negative effects of AD pathology on AD dementia proximate to death (OR 0.70, SE 0.14, = 0.010). Up to 90% of cognitive resilience peptides were related to AD pathologic phenotypes.
Cortical proteins may provide some degree of cognitive resilience. These multifunctional proteins also seem to provide resilience to other AD clinical phenotypes and have independent associations with ADRD pathologies. Resilience proteins may be high-value therapeutic targets for drug discovery of interventions that maintain brain health in aging adults via multiple pathways.
认知弹性(resilience)是一个公认的概念,但由于对其潜在机制的了解不足,使得开发能够识别具有高或低弹性的老年人的工具变得困难。我们测试了将与认知弹性相关的皮质肽聚合到一个指数中是否可以识别出具有更高或更低认知弹性的成年人。
我们使用了来自 1192 名已故老年人的数据,包括年度临床测试、10 种阿尔茨海默病(AD)和相关痴呆症(ADRD)病理指标,以及在背外侧前额叶皮层测量的 226 种蛋白肽。我们使用线性混合效应模型来识别与认知弹性相关的肽(即,认知衰退不能用 ADRD 病理来解释[错误发现率<0.05])。我们将这些弹性肽的表达水平聚合到一个特定于人的认知弹性指数中,并研究了它与 AD 临床和病理表型的关联。
我们从与认知弹性相关的 226 种肽中构建了一个弹性指数。更高的指数与更缓慢的认知衰退(估计值为 0.05,SE 为 0.003,<0.001)和更缓慢的运动衰退(估计值为 0.005,SE 为 0.001,<0.001)相关。大多数弹性肽(70%)是专门针对认知衰退的,但 30%也为运动衰退提供了弹性。更高的指数也与 AD 病理负担较低相关(比值比[OR]为 0.41,SE 为 0.01,<0.001),并改变了 AD 病理与认知的关联,即更高的指数改变了 AD 病理对接近死亡时 AD 痴呆的负面影响(OR 为 0.70,SE 为 0.14,=0.010)。高达 90%的认知弹性肽与 AD 病理表型有关。
皮质蛋白可能提供一定程度的认知弹性。这些多功能蛋白似乎也为其他 AD 临床表型提供了弹性,并且与 ADRD 病理有独立的关联。弹性蛋白可能是通过多种途径维持老年人大脑健康的干预药物发现的高价值治疗靶点。