Department of Biomedical Informatics, The Ohio State University College of Medicine, Lincoln Tower, 1800 Cannon Drive, Columbus, OH, 43210, USA.
Parent Project Muscular Dystrophy, Washington, DC, USA.
Patient. 2022 Sep;15(5):577-588. doi: 10.1007/s40271-022-00574-y. Epub 2022 Mar 4.
Caregivers routinely inform medical and regulatory decision making in rare pediatric diseases. While differences in treatment preferences across caregivers and patients have been observed for Duchenne muscular dystrophy, this evidence was limited by small samples of patients and results were confounded by patient age and disease progression. We tested caregiver and patient preference concordance for treating Duchenne.
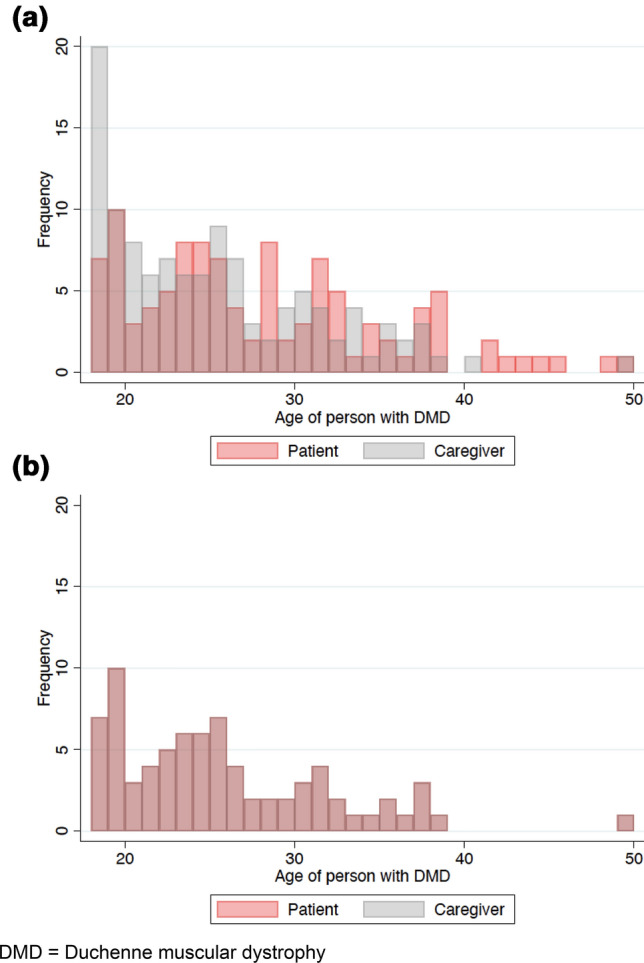
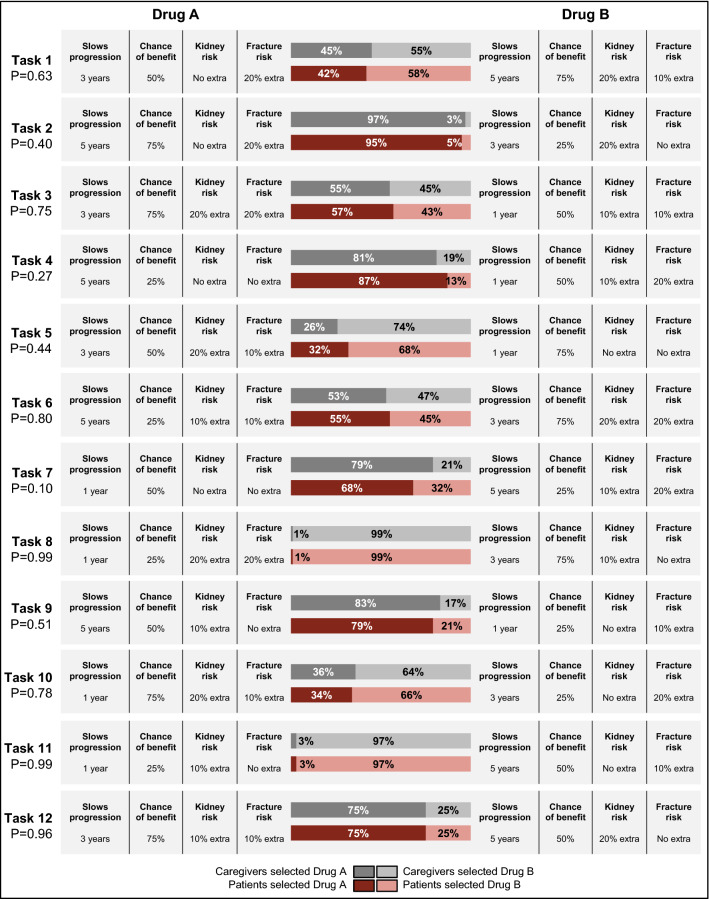
Preferences and demographic/clinical information from 115 caregivers and 107 patients were collected in an international study (response = 80%) using a previously developed discrete-choice experiment consisting of 12 experimentally controlled choice tasks. Each task presented two profiles that varied across four attributes: disease progression, drug failure probability, kidney damage risk, and fracture risk. Caregivers and patients were matched 1:1 based on patient age. We tested for concordance across each task and by comparing caregivers' and patients' maximum acceptable risk of drug failure, kidney damage, and fracture for a slowing of disease progression.
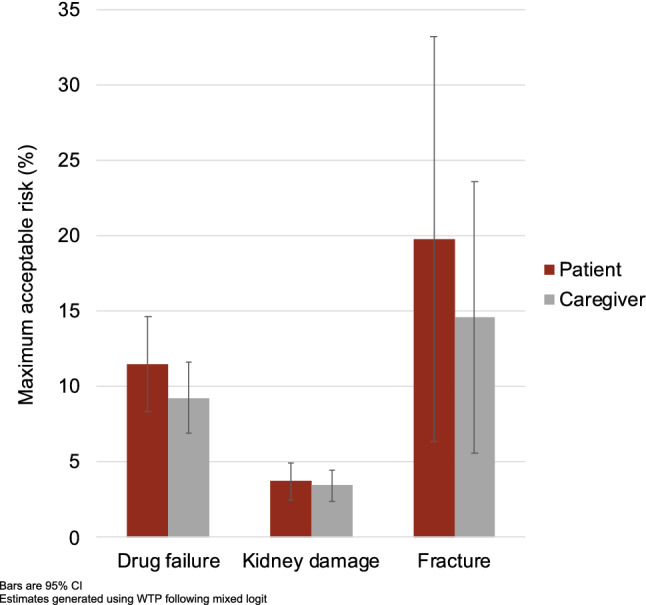
The final analysis included 77 caregivers and 77 patients. No differences were observed in nationality (p = 0.969), disease stage (p = 0.180), or demographic/clinical factors (p = 0.093-0.857); however, patients were more optimistic (p = 0.030). Caregivers and patients chose similarly across tasks (p = 0.101-0.993). To slow disease progression by 1 year, caregivers and patients would tolerate a 9% and 11% increase in drug failure probability, respectively (p = 0.267). Alternatively, they would accept a 3% and 4% increase in the risk of kidney damage (p = 0.719) or a 15% and 20% increase in the risk of fracture (p = 0.534).
Caregivers and patients had concordant preferences for treating Duchenne. Providers and regulators can trust both caregiver and patient report of preferences to inform medical decision making.
在罕见儿科疾病中,护理人员经常为医疗和监管决策提供信息。尽管已经观察到在杜氏肌营养不良症中,护理人员和患者的治疗偏好存在差异,但由于患者样本量小且结果受到患者年龄和疾病进展的影响,这一证据受到限制。我们测试了治疗杜氏肌营养不良症的护理人员和患者的偏好一致性。
在一项国际研究中,通过先前开发的包含 12 个实验控制选择任务的离散选择实验,收集了 115 名护理人员和 107 名患者的偏好和人口统计学/临床信息(应答率为 80%)。每个任务呈现两个在四个属性上变化的档案:疾病进展、药物失败概率、肾脏损伤风险和骨折风险。根据患者年龄,护理人员和患者进行一对一匹配。我们测试了每个任务以及护理人员和患者对药物失败、肾脏损伤和骨折的最大可接受风险的比较,以减缓疾病进展。
最终分析包括 77 名护理人员和 77 名患者。在国籍(p = 0.969)、疾病阶段(p = 0.180)或人口统计学/临床因素(p = 0.093-0.857)方面没有差异;然而,患者更为乐观(p = 0.030)。护理人员和患者在任务中选择相似(p = 0.101-0.993)。为了使疾病进展延缓 1 年,护理人员和患者分别将容忍药物失败概率增加 9%和 11%(p = 0.267)。或者,他们将接受肾脏损伤风险增加 3%和 4%(p = 0.719)或骨折风险增加 15%和 20%(p = 0.534)。
护理人员和患者对治疗杜氏肌营养不良症的偏好具有一致性。提供者和监管机构可以信任护理人员和患者报告的偏好,以告知医疗决策。