College of Pharmacy, University of South Carolina, Columbia, SC, USA.
Acadia Pharmaceuticals, Inc, San Diego, CA, USA.
Adv Ther. 2022 May;39(5):1993-2008. doi: 10.1007/s12325-022-02075-8. Epub 2022 Mar 5.
Dementia-related psychosis (DRP) is characterized by hallucinations and delusions, which may increase the debilitating effects of underlying dementia. This network meta-analysis (NMA) evaluated the comparative efficacy, safety, and acceptability of atypical antipsychotics (AAPs) commonly used off label to treat DRP.
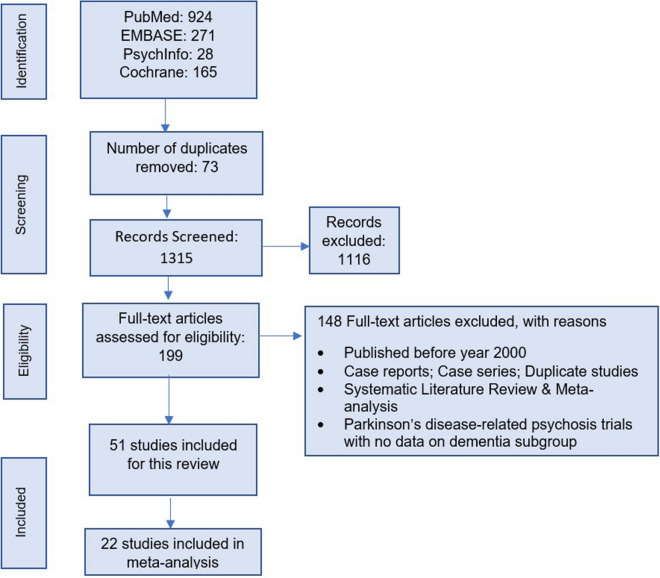
We included 22 eligible studies from a systematic literature review of AAPs (quetiapine, risperidone, olanzapine, aripiprazole, and brexpiprazole) used off label to treat DRP. Study outcomes were: (1) efficacy-neuropsychiatric inventory-nursing home (NPI-NH psychosis subscale), (2) safety-mortality, cerebrovascular events (CVAEs), and others (somnolence, falls, fractures, injuries, etc.), and (3) acceptability-discontinuations due to all causes, lack of efficacy, and adverse events (AEs). We used random-effects modeling to estimate pooled standardized mean differences (SMDs) for NPI-NH psychosis subscale scores and odds ratios (OR) for other dichotomous outcomes, with their respective 95% confidence intervals (CIs).
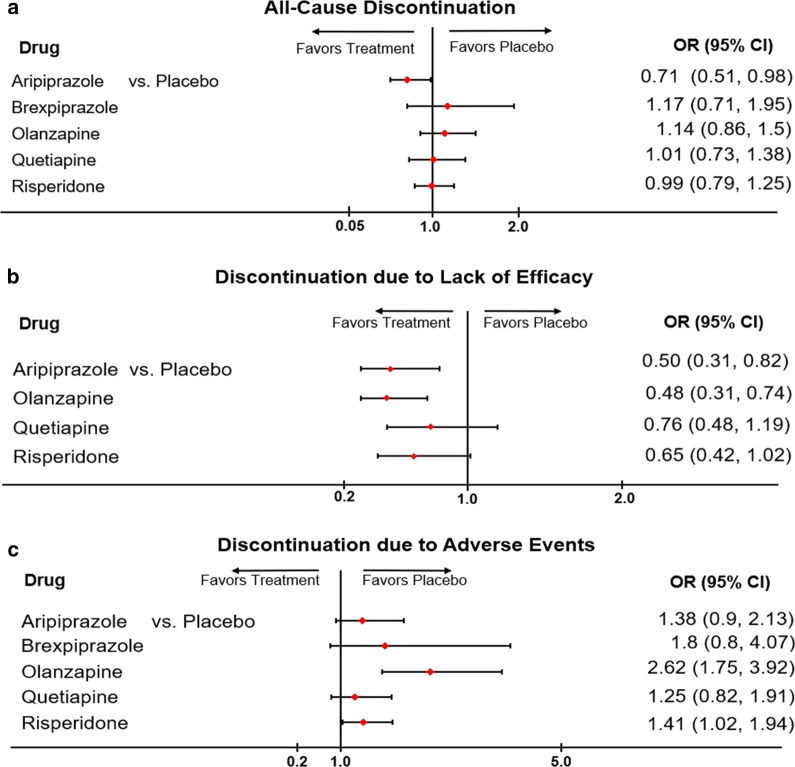
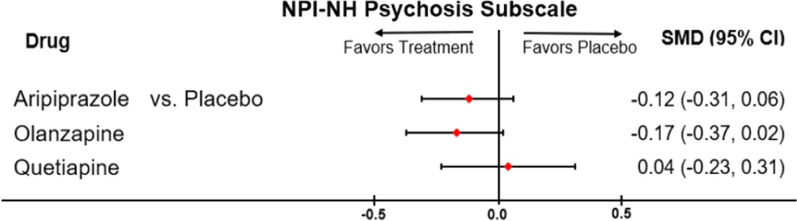
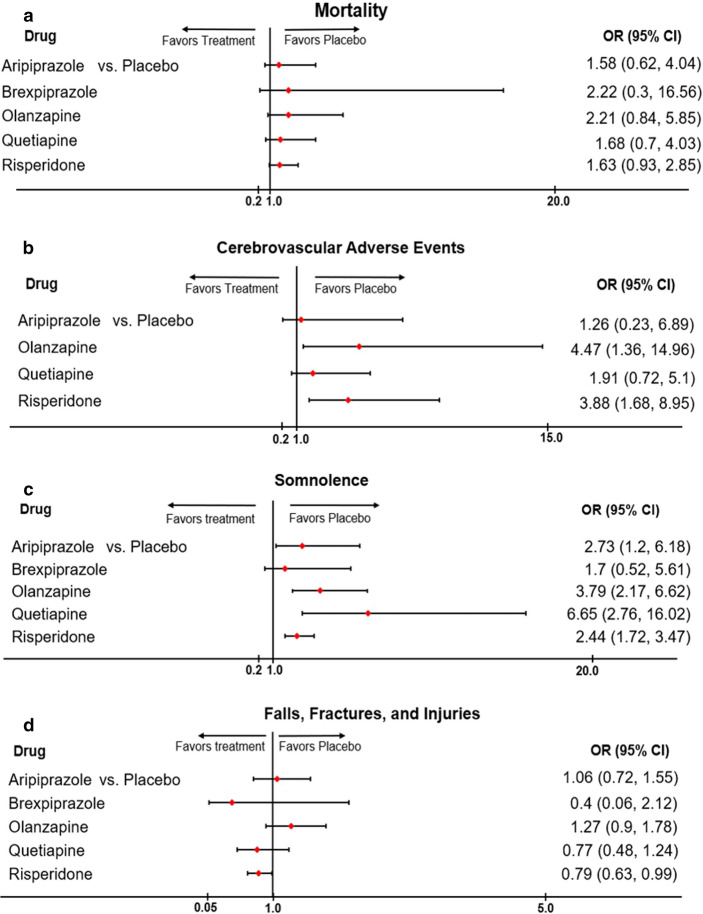
Compared with placebo, aripiprazole (SMD - 0.12; 95% CI - 0.31, 0.06), and olanzapine (SMD - 0.17; 95% CI - 0.04; 0.02) demonstrated small, non-significant numerical improvements in NPI-NH psychosis scores (5 studies; n = 1891), while quetiapine (SMD 0.04; 95% CI - 0.23, 0.32) did not improve symptoms. The odds of mortality (15 studies, n = 4989) were higher for aripiprazole (OR 1.58; 95% CI 0.62, 4.04), brexpiprazole (OR 2.22; 95% CI 0.30, 16.56), olanzapine (OR 2.21; 95% CI 0.84, 5.85), quetiapine (OR 1.68; 95% CI 0.70, 4.03), and risperidone (OR 1.63; 95% CI 0.93, 2.85) than for placebo. Risperidone (OR 3.68; 95% CI 1.68, 8.95) and olanzapine (OR 4.47; 95% CI 1.36, 14.69) demonstrated significantly greater odds of CVAEs compared to placebo. Compared with placebo, odds of all-cause discontinuation were significantly lower for aripiprazole (OR 0.71; 95% CI 0.51, 0.98; 20 studies; 5744 patients) and higher for other AAPs. Aripiprazole (OR 0.5; 95% CI 0.31, 0.82) and olanzapine (OR 0.48; 95% CI 0.31, 0.74) had significantly lower odds of discontinuation due to lack of efficacy (OR 12 studies; n = 4382) compared to placebo, while results for quetiapine and risperidone were not significant. Compared with placebo, the odds of discontinuation due to AEs (19 studies, n = 5445) were higher for olanzapine (OR 2.62; 95% CI 1.75, 3.92), brexpiprazole (OR 1.80; 95% CI 0.80, 4.07), quetiapine (OR 1.25; 95% CI 0.82, 1.91), aripiprazole (OR 1.38; 95% CI 0.90, 2.13), and risperidone (OR 1.41; 95% CI 1.02, 1.94).
Overall results demonstrate that, compared with placebo, quetiapine is not associated with improvement in psychosis in patients with dementia, while olanzapine and aripiprazole have non-significant small numerical improvements. These off-label AAPs (quetiapine, risperidone, olanzapine, aripiprazole, and brexpiprazole) are associated with greater odds of mortality, CVAEs, and discontinuations due to AEs than placebo. These results underscore the ongoing unmet need for newer pharmacological options with a more favorable benefit-risk profile for the treatment of DRP.
痴呆相关精神病(DRP)的特征是幻觉和妄想,这可能会加重潜在痴呆症的致残影响。本网络荟萃分析(NMA)评估了通常被标签外用于治疗 DRP 的几种非典型抗精神病药(AAP)的疗效、安全性和可接受性。
我们从 AAP(喹硫平、利培酮、奥氮平、阿立哌唑和布瑞哌唑)治疗 DRP 的系统文献综述中纳入了 22 项合格研究。研究结果为:(1)疗效-神经精神病学入院护理院(NPI-NH 精神病亚量表),(2)安全性-死亡率、脑血管事件(CVAEs)和其他(嗜睡、跌倒、骨折、损伤等),以及(3)可接受性-因所有原因、缺乏疗效和不良事件(AE)而停药。我们使用随机效应模型估计 NPI-NH 精神病亚量表评分的标准化均数差(SMD)和其他二分类结局的比值比(OR),并分别给出其 95%置信区间(CI)。
与安慰剂相比,阿立哌唑(SMD -0.12;95%CI -0.31,0.06)和奥氮平(SMD -0.17;95%CI -0.04;0.02)在 NPI-NH 精神病评分方面有较小但无统计学意义的数值改善(5 项研究;n=1891),而喹硫平(SMD 0.04;95%CI -0.23,0.32)并未改善症状。阿立哌唑(OR 1.58;95%CI 0.62,4.04)、布瑞哌唑(OR 2.22;95%CI 0.30,16.56)、奥氮平(OR 2.21;95%CI 0.84,5.85)、喹硫平(OR 1.68;95%CI 0.70,4.03)和利培酮(OR 1.63;95%CI 0.93,2.85)的死亡率高于安慰剂。利培酮(OR 3.68;95%CI 1.68,8.95)和奥氮平(OR 4.47;95%CI 1.36,14.69)发生 CVAEs 的几率明显高于安慰剂。与安慰剂相比,阿立哌唑(OR 0.71;95%CI 0.51,0.98;20 项研究;5744 例患者)和其他 AAP 的全因停药几率较低,而其他 AAP 的停药几率较高。阿立哌唑(OR 0.5;95%CI 0.31,0.82)和奥氮平(OR 0.48;95%CI 0.31,0.74)因缺乏疗效而停药的几率明显低于安慰剂(OR 12 项研究;n=4382),而喹硫平和利培酮的结果则不显著。与安慰剂相比,奥氮平(OR 2.62;95%CI 1.75,3.92)、布瑞哌唑(OR 1.80;95%CI 0.80,4.07)、喹硫平(OR 1.25;95%CI 0.82,1.91)、阿立哌唑(OR 1.38;95%CI 0.90,2.13)和利培酮(OR 1.41;95%CI 1.02,1.94)因 AE 而停药的几率较高。
总体结果表明,与安慰剂相比,喹硫平与痴呆患者的精神病改善无关,而奥氮平和阿立哌唑则有较小但无统计学意义的数值改善。这些标签外的 AAP(喹硫平、利培酮、奥氮平、阿立哌唑和布瑞哌唑)与安慰剂相比,死亡率、CVAEs 和因 AE 而停药的几率更高。这些结果强调了对治疗 DRP 的新型药理学选择的持续需求,这种选择具有更有利的风险效益比。