Department of Radiation Oncology, Amsterdam University Medical Centers, Vrije Universiteit Amsterdam, Cancer Center Amsterdam, Amsterdam, The Netherlands.
Istanbul University-Cerrahpaşa, Cerrahpaşa School of Medicine, Istanbul, Turkey.
ESMO Open. 2022 Apr;7(2):100410. doi: 10.1016/j.esmoop.2022.100410. Epub 2022 Mar 2.
The phase III PACIFIC trial (NCT02125461) established consolidation durvalumab as standard of care for patients with unresectable, stage III non-small-cell lung cancer (NSCLC) and no disease progression following chemoradiotherapy (CRT). In some cases, patients with stage IIIA-N2 NSCLC are considered operable, but the relative benefit of surgery is unclear. We report a post hoc, exploratory analysis of clinical outcomes in the PACIFIC trial, in patients with or without stage IIIA-N2 NSCLC.
Patients with unresectable, stage III NSCLC and no disease progression after ≥2 cycles of platinum-based, concurrent CRT were randomized 2 : 1 to receive durvalumab (10 mg/kg intravenously; once every 2 weeks for up to 12 months) or placebo, 1-42 days after CRT. The primary endpoints were progression-free survival (PFS; assessed by blinded independent central review according to RECIST version 1.1) and overall survival (OS). Treatment effects within subgroups were estimated by hazard ratios (HRs) from unstratified Cox proportional hazards models.
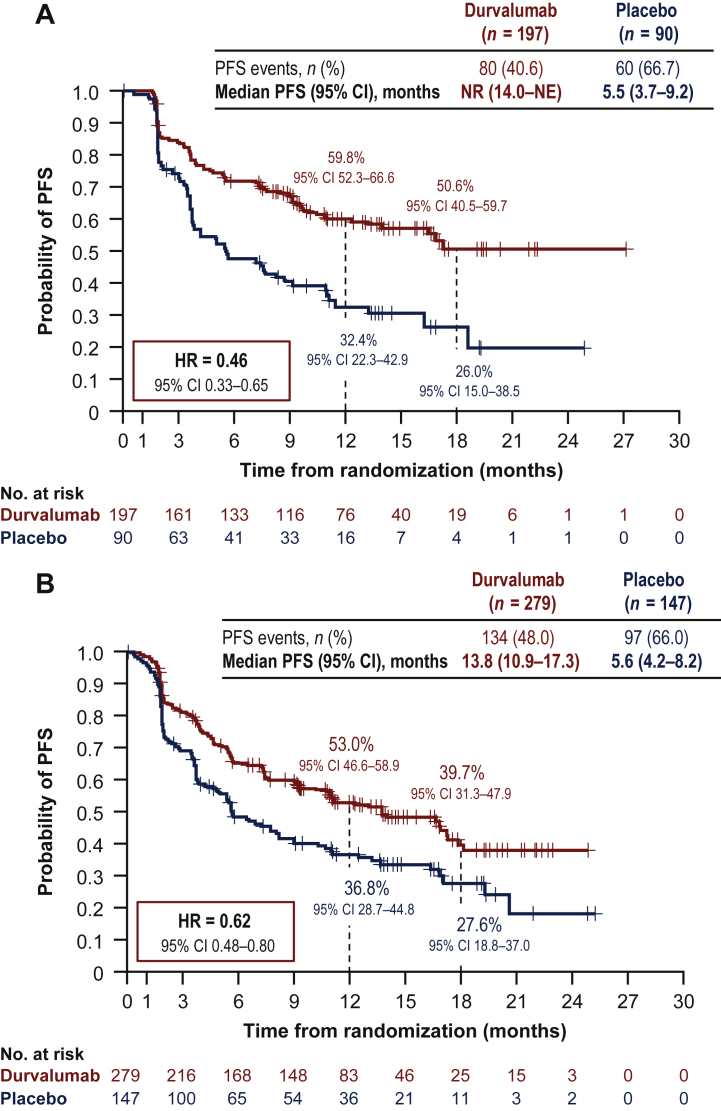
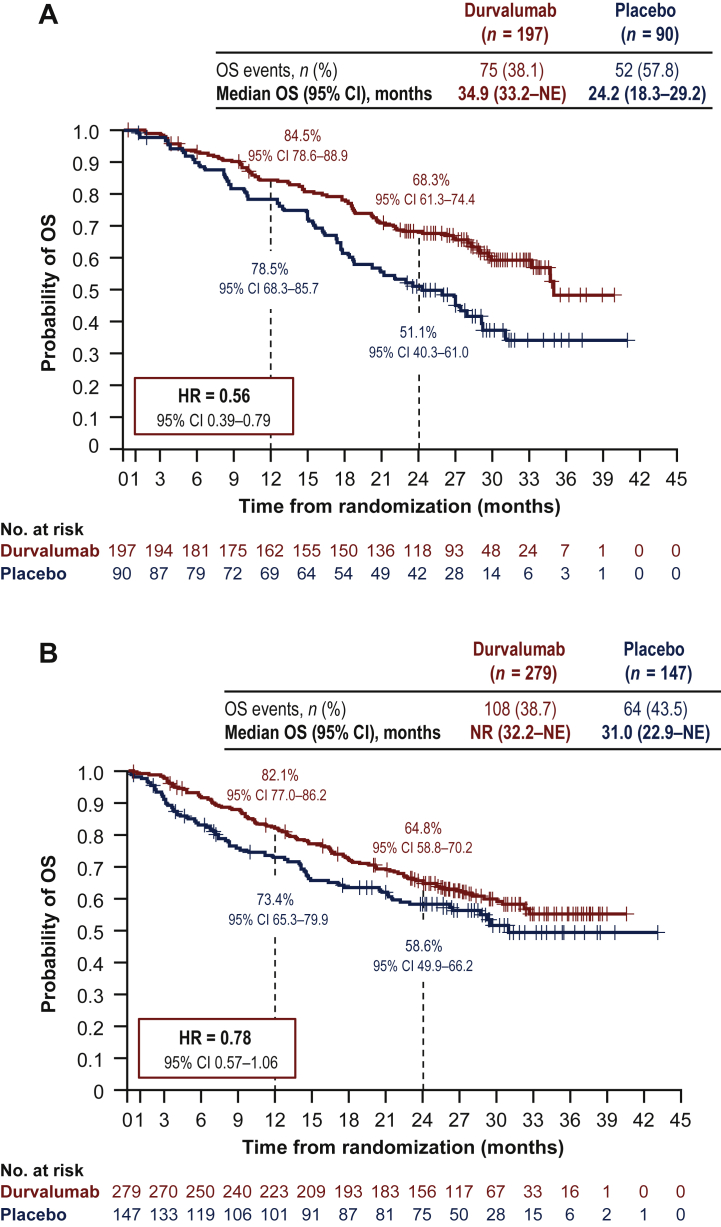
Of 713 randomized patients, 287 (40%) had stage IIIA-N2 disease. Baseline characteristics were similar between patients with and without stage IIIA-N2 NSCLC. With a median follow-up of 14.5 months (range: 0.2-29.9 months), PFS was improved with durvalumab versus placebo in both patients with [HR = 0.46; 95% confidence interval (CI), 0.33-0.65] and without (HR = 0.62; 95% CI 0.48-0.80) stage IIIA-N2 disease. Similarly, with a median follow-up of 25.2 months (range: 0.2-43.1 months), OS was improved with durvalumab versus placebo in patients with (HR = 0.56; 95% CI 0.39-0.79) or without (HR = 0.78; 95% CI 0.57-1.06) stage IIIA-N2 disease. Durvalumab had a manageable safety profile irrespective of stage IIIA-N2 status.
Consistent with the intent-to-treat population, treatment benefits with durvalumab were confirmed in patients with stage IIIA-N2, unresectable NSCLC. Prospective studies are needed to determine the optimal treatment approach for patients who are deemed operable.
III 期 PACIFIC 试验(NCT02125461)确立了巩固性 durvalumab 治疗用于不可切除的 III 期非小细胞肺癌(NSCLC)患者的标准治疗方案,这些患者在接受放化疗(CRT)后无疾病进展。在某些情况下,III 期 N2 期 NSCLC 患者被认为具有手术指征,但手术的相对获益尚不清楚。我们报告了 PACIFIC 试验的一项事后探索性分析结果,评估了接受或不接受 III 期 N2 期 NSCLC 治疗的患者的临床结局。
不可切除的 III 期 NSCLC 患者,在接受至少 2 个周期含铂类药物的同期 CRT 后无疾病进展,随机接受 durvalumab(10mg/kg 静脉注射;每 2 周 1 次,最多 12 个月)或安慰剂治疗,在 CRT 后 1-42 天内进行。主要终点为无进展生存期(PFS;根据 RECIST 版本 1.1 进行盲法独立中心评估)和总生存期(OS)。通过非分层 Cox 比例风险模型的风险比(HR)来估计亚组内的治疗效果。
713 例随机患者中,287 例(40%)患有 IIIA-N2 期疾病。有和无 IIIA-N2 期 NSCLC 的患者的基线特征相似。中位随访 14.5 个月(范围:0.2-29.9 个月),durvalumab 组较安慰剂组在有和无 IIIA-N2 期疾病的患者中均显著改善了 PFS[HR 分别为 0.46(95%置信区间:0.33-0.65)和 0.62(95%置信区间:0.48-0.80)]。同样,中位随访 25.2 个月(范围:0.2-43.1 个月),durvalumab 组较安慰剂组在有和无 IIIA-N2 期疾病的患者中均显著改善了 OS[HR 分别为 0.56(95%置信区间:0.39-0.79)和 0.78(95%置信区间:0.57-1.06)]。无论 IIIA-N2 期状态如何,durvalumab 的安全性均可控。
与意向治疗人群一致,durvalumab 治疗在 IIIA-N2 期不可切除 NSCLC 患者中得到了确认。需要前瞻性研究来确定对于那些被认为具有手术指征的患者的最佳治疗方法。