Cha Jung-Joon, Kim Jong-Youn, Kim Hyoeun, Ko Young-Guk, Choi Donghoon, Lee Jae-Hwan, Yoon Chang-Hwan, Chae In-Ho, Yu Cheol Woong, Lee Seung Whan, Lee Sang-Rok, Choi Seung Hyuk, Koh Yoon Seok, Min Pil-Ki
Division of Cardiology, Department of Internal Medicine, Korea University Anam Hospital, Seoul, Korea.
Division of Cardiology, Department of Internal Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
Korean Circ J. 2022 Jun;52(6):429-440. doi: 10.4070/kcj.2021.0342. Epub 2022 Feb 10.
Endovascular therapy (EVT) first strategy has been widely adopted for the treatment of chronic limb threatening ischemia (CLTI) patients in real-world practice. This study aimed to investigate long-term outcomes of CLTI patients who underwent EVT and identify prognostic factors.
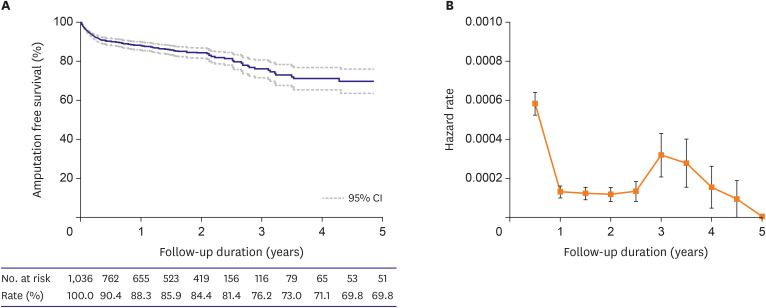
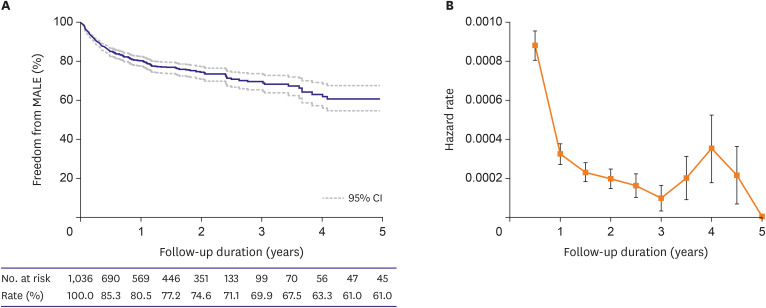
From the retrospective cohorts of a Korean multicenter endovascular therapy registry, 1,036 patients with CLTI (792 men, 68.8 ± 9.5 years) were included. The primary endpoint was amputation-free survival (AFS) defined as the absence of major amputation or death. Secondary endpoints were major adverse limb events (MALE; a composite of major amputation, minor amputation, and reintervention).
Five-year AFS and freedom from MALE were 69.8% and 61%, respectively. After multivariate analysis, age (hazard ratio [HR], 1.476; p<0.001), end-stage renal disease (ESRD; HR, 2.340; p<0.001), Rutherford category (RC) 6 (HR, 1.456; p=0.036), and suboptimal EVT (HR, 1.798; p=0.005) were identified as predictors of major amputation or death, whereas smoking (HR, 0.594; p=0.007) was protective. Low body mass index (HR, 1.505; p=0.046), ESRD (HR, 1.648; p=0.001), femoropopliteal lesion (HR, 1.877; p=0.004), RC-6 (HR, 1.471; p=0.008), and suboptimal EVT (HR, 1.847; p=0.001) were predictors of MALE. The highest hazard rates were observed during the first 6 months for both major amputation or death and MALE. After that, the hazard rate decreased and rose again after 3-4 years.
In CLTI patients, long-term outcomes of EVT were acceptable. ESRD, RC-6, and suboptimal EVT were common predictors for poor clinical outcomes.
ClinicalTrials.gov Identifier: NCT02748226.
在实际临床实践中,血管内治疗(EVT)优先策略已被广泛应用于治疗严重肢体缺血(CLTI)患者。本研究旨在探讨接受EVT治疗的CLTI患者的长期预后,并确定预后因素。
从韩国多中心血管内治疗登记处的回顾性队列中,纳入1036例CLTI患者(792例男性,年龄68.8±9.5岁)。主要终点是无截肢生存(AFS),定义为无大截肢或死亡。次要终点是主要肢体不良事件(MALE;大截肢、小截肢和再次干预的复合事件)。
5年AFS率和无MALE事件生存率分别为69.8%和61%。多因素分析后,年龄(风险比[HR],1.476;p<0.001)、终末期肾病(ESRD;HR,2.340;p<0.001)、卢瑟福分级(RC)6级(HR,1.456;p=0.036)和非最佳EVT(HR,1.798;p=0.005)被确定为大截肢或死亡的预测因素,而吸烟(HR,0.594;p=0.007)具有保护作用。低体重指数(HR,1.505;p=0.046)、ESRD(HR,1.648;p=0.001)、股腘动脉病变(HR,1.877;p=)、RC-6级(HR,1.471;p=0.008)和非最佳EVT(HR,1.847;p=0.001)是MALE的预测因素。大截肢或死亡和MALE在最初6个月内的风险率最高。此后,风险率下降,并在3-4年后再次上升。
在CLTI患者中,EVT的长期预后是可以接受的。ESRD、RC-6级和非最佳EVT是临床预后不良的常见预测因素。
ClinicalTrials.gov标识符:NCT02748226。