National Heart and Lung Institute, Imperial College London, London, UK.
Epidemiology, AstraZeneca, Cambridge, UK.
Int J Chron Obstruct Pulmon Dis. 2022 Mar 3;17:427-437. doi: 10.2147/COPD.S346591. eCollection 2022.
Studies have shown that chronic obstructive pulmonary disease (COPD) exacerbation events are related to future events; however, previous literature typically reports frequent vs infrequent exacerbations per patient-year and no studies have investigated increasing number of severe exacerbations in relation to COPD outcomes.
To investigate the association between baseline frequency and severity of exacerbations and subsequent mortality and exacerbation risk in a COPD cohort.
Clinical Practice Research Datalink (CPRD) Aurum and Hospital Episode Statistics data were used to identify patients registered at general practices in the UK, who had a diagnosis of COPD, were over the age of 40 years, were smokers or ex-smokers and had data recorded from 2004 onwards. Frequency and severity of exacerbations in the baseline year were identified as moderate exacerbations (general practice events) and severe exacerbations (hospitalised events). Patients were categorised as having: none, 1 moderate only, 2 moderate only, 3+ moderate only, 1 severe (and any moderate), 2 severe (and any moderate), and 3+ severe (and any moderate exacerbations). Poisson regression was used to investigate the association between baseline exacerbation frequency/severity and exacerbation events and mortality over follow-up.
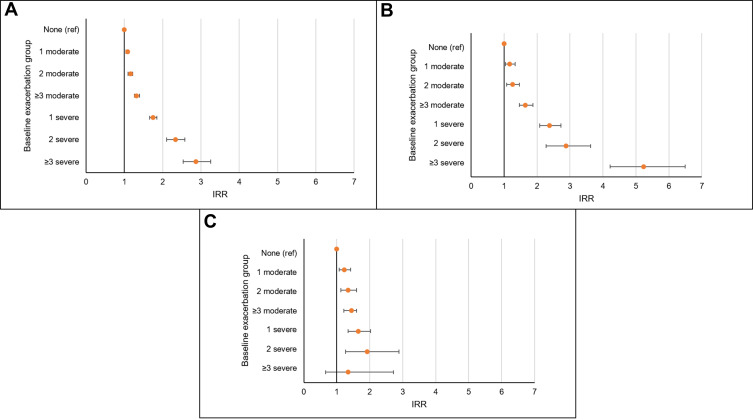
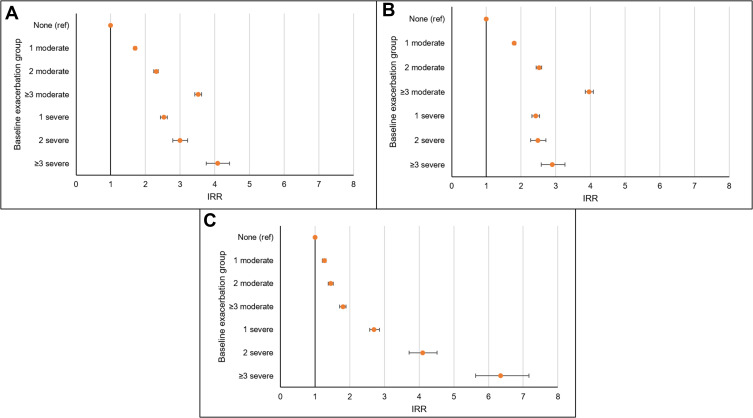
Overall, 340,515 COPD patients were included. Patients had higher rates of future exacerbations with increasing frequency and severity of baseline exacerbations compared to no baseline exacerbations. Adjusted incidence rate ratios (IRR) for patients with 1, 2, and 3+ moderate exacerbations compared to 0 exacerbations were 1.70 (95% CI 1.66-1.74), 2.31 (95% CI 2.24-2.37), and 3.52 (95% CI 3.43-3.62), respectively. Patients with increased frequency of baseline exacerbations were more likely to die from all-cause, COPD-related, and cardiovascular-related mortality in a graduated fashion.
Increasing number and severity of exacerbations were associated with increasing risk of subsequent exacerbations, all-cause mortality and COPD-related mortality. Even a single moderate event increases the risk of future events, illustrating that every exacerbation counts.
研究表明,慢性阻塞性肺疾病(COPD)加重事件与未来事件有关;然而,以前的文献通常报告每位患者每年的频繁加重与不频繁加重,并且没有研究调查与 COPD 结局相关的严重加重次数的增加。
在 COPD 队列中调查基线加重频率和严重程度与随后的死亡率和加重风险之间的关系。
使用临床实践研究数据库(CPRD)Aurum 和医院病例统计数据,确定在英国普通诊所登记的患有 COPD 的患者,年龄超过 40 岁,是吸烟者或前吸烟者,并且从 2004 年开始有数据记录。基线年内的加重频率和严重程度被确定为中度加重(普通实践事件)和重度加重(住院事件)。患者被分为以下几类:无,1 次中度加重,2 次中度加重,3 次或以上中度加重,1 次重度加重(并伴有任何中度加重),2 次重度加重(并伴有任何中度加重),3 次或以上重度加重(并伴有任何中度加重)。泊松回归用于调查基线加重频率/严重程度与随访期间加重事件和死亡率之间的关系。
总体而言,纳入了 340515 名 COPD 患者。与没有基线加重的患者相比,基线加重频率和严重程度较高的患者未来加重的发生率更高。与没有加重的患者相比,基线时有 1 次、2 次和 3 次或以上中度加重的患者的调整后的发生率比值比(IRR)分别为 1.70(95%CI 1.66-1.74)、2.31(95%CI 2.24-2.37)和 3.52(95%CI 3.43-3.62)。基线加重频率增加的患者死于全因、COPD 相关和心血管相关死亡率的可能性呈梯度增加。
加重次数和严重程度的增加与随后加重、全因死亡率和 COPD 相关死亡率的风险增加相关。即使是单次中度加重也会增加未来事件的风险,这表明每次加重都很重要。