Moffitt Cancer Center, Tampa, Florida.
JAMA Oncol. 2022 May 1;8(5):748-754. doi: 10.1001/jamaoncol.2022.0001.
Patients with cancer experience high rates of morbidity and mortality after SARS-CoV-2 infection. Immune response to mRNA-1273 vaccination across multiple cancer types and treatments remains to be established.
To quantitate antibody responses after mRNA-1273 vaccination among patients with solid tumors and hematologic cancer and to assess clinical and treatment factors associated with vaccine response.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study included patients with cancer who were aged 18 years or older, spoke English or Spanish, had received their first mRNA-1273 dose between January 12 and 25, 2021, and agreed to blood tests before and after vaccination.
Receipt of 1 and 2 mRNA-1273 SARS-CoV-2 vaccine doses.
Seroconversion after each vaccine dose and IgG levels against SARS-CoV-2 spike protein obtained immediately before the first and second vaccine doses and 57 days (plus or minus 14 days) after the first vaccine dose. Cancer diagnoses and treatments were ascertained by medical record review. Serostatus was assessed via enzyme-linked immunosorbent assay. Paired t tests were applied to examine days 1, 29, and 57 SARS-CoV-2 antibody levels. Binding antibody IgG geometric mean titers were calculated based on log10-transformed values.
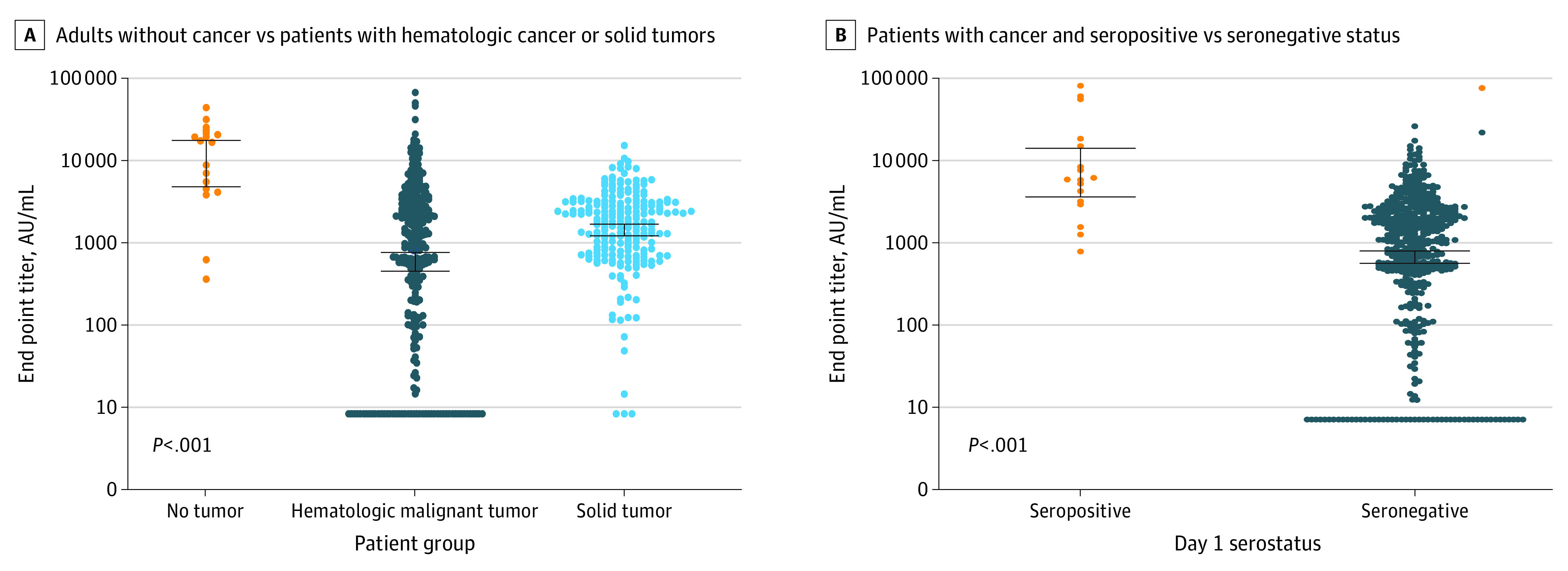
The 515 participants were a mean (SD) age of 64.5 (11.4) years; 262 (50.9%) were women; and 32 (6.2%) were Hispanic individuals and 479 (93.0%) White individuals; race and ethnicity data on 4 (0.7%) participants were missing. Seropositivity after vaccine dose 2 was 90.3% (465; 95% CI, 87.4%-92.7%) among patients with cancer, was significantly lower among patients with hematologic cancer (84.7% [255]; 95% CI, 80.1%-88.6%) vs solid tumors (98.1% [210]; 95% CI, 95.3%-99.5%), and was lowest among patients with lymphoid cancer (70.0% [77]; 95% CI, 60.5%-78.4%). Patients receiving a vaccination within 6 months after anti-CD20 monoclonal antibody treatment had a significantly lower seroconversion (6.3% [1]; 95% CI, 0.2%-30.2%) compared with those treated 6 to 24 months earlier (53.3% [8]; 95% CI, 26.6%-78.7%) or those who never received anti-CD20 treatment (94.2% [456]; 95% CI, 91.7%-96.1%). Low antibody levels after vaccination were observed among patients treated with anti-CD20 within 6 months before vaccination (GM, 15.5 AU/mL; 95% CI, 9.8-24.5 AU/mL), patients treated with small molecules (GM, 646.7 AU/mL; 95% CI, 441.9-946.5 AU/mL), and patients with low lymphocyte (GM, 547.4 AU/mL; 95% CI, 375.5-797.7 AU/mL) and IgG (GM, 494.7 AU/mL; 95% CI, 304.9-802.7 AU/mL) levels.
This cohort study found that the mRNA-1273 SARS-CoV-2 vaccine induced variable antibody responses that differed by cancer diagnosis and treatment received. These findings suggest that patients with hematologic cancer and those who are receiving immunosuppressive treatments may need additional vaccination doses.
癌症患者在感染 SARS-CoV-2 后发病率和死亡率较高。mRNA-1273 疫苗在多种癌症类型和治疗中的免疫反应仍有待确定。
定量评估实体瘤和血液癌患者接受 mRNA-1273 疫苗接种后的抗体反应,并评估与疫苗反应相关的临床和治疗因素。
设计、地点和参与者:这项队列研究纳入了年龄在 18 岁或以上、会说英语或西班牙语、在 2021 年 1 月 12 日至 25 日之间接受了第一剂 mRNA-1273 疫苗且同意在接种前后进行血液检测的癌症患者。
接受 1 剂和 2 剂 SARS-CoV-2 mRNA-1273 疫苗。
每剂疫苗接种后的血清转化率以及在第一剂和第二剂疫苗接种前以及第一剂疫苗接种后 57 天(加减 14 天)获得的 SARS-CoV-2 刺突蛋白 IgG 水平。通过病历回顾确定癌症诊断和治疗。通过酶联免疫吸附试验评估血清状态。应用配对 t 检验来检测第 1、29 和 57 天的 SARS-CoV-2 抗体水平。根据 log10 转换值计算结合抗体 IgG 几何平均滴度。
515 名参与者的平均(SD)年龄为 64.5(11.4)岁;262 名(50.9%)为女性;32 名(6.2%)为西班牙裔个体,479 名(93.0%)为白人个体;4 名(0.7%)参与者的种族和民族数据缺失。癌症患者中,第 2 剂疫苗接种后的血清阳性率为 90.3%(465;95% CI,87.4%-92.7%),血液癌患者(84.7%[255];95% CI,80.1%-88.6%)显著低于实体瘤患者(98.1%[210];95% CI,95.3%-99.5%),淋巴癌患者最低(70.0%[77];95% CI,60.5%-78.4%)。与接受抗 CD20 单克隆抗体治疗 6 至 24 个月或从未接受过抗 CD20 治疗的患者(分别为 53.3%[8]和 94.2%[456])相比,在接受抗 CD20 治疗后 6 个月内接受疫苗接种的患者血清转化率显著较低(6.3%[1];95% CI,0.2%-30.2%)。在接种疫苗后,接受抗 CD20 治疗 6 个月内的患者抗体水平较低(GM,15.5 AU/mL;95% CI,9.8-24.5 AU/mL)、接受小分子治疗的患者(GM,646.7 AU/mL;95% CI,441.9-946.5 AU/mL)和淋巴细胞(GM,547.4 AU/mL;95% CI,375.5-797.7 AU/mL)和 IgG(GM,494.7 AU/mL;95% CI,304.9-802.7 AU/mL)水平较低的患者。
这项队列研究发现,mRNA-1273 SARS-CoV-2 疫苗诱导了不同的抗体反应,这些反应因癌症诊断和接受的治疗而异。这些发现表明,血液癌患者和接受免疫抑制治疗的患者可能需要额外的疫苗剂量。