Shah Manish A, Udrea Anghel Adrian, Bondarenko Igor, Mansoor Was, Sánchez Raquel Guardeño, Sarosiek Tomasz, Bozzarelli Silvia, Schenker Michael, Gomez-Martin Carlos, Morgan Carys, Özgüroğlu Mustafa, Pikiel Joanna, Kalofonos Haralabos P, Wojcik Elzbieta, Buchler Tomas, Swinson Daniel, Cicin Irfan, Joseph Mano, Vynnychenko Ihor, Luft Alexander Valerievich, Enzinger Peter C, Salek Tomas, Papandreou Christos, Tournigand Christophe, Maiello Evaristo, Wei Ran, Ferry David, Gao Ling, Oliveira Joana M, Ajani Jaffer A
Department of Medicine, Division of Hematology and Medical Oncology, Weill Cornell Medical College, New York, NY 10021, USA.
Cancer Center, Medisprof SRL, 400641 Cluj-Napoca, Romania.
Cancers (Basel). 2022 Feb 24;14(5):1168. doi: 10.3390/cancers14051168.
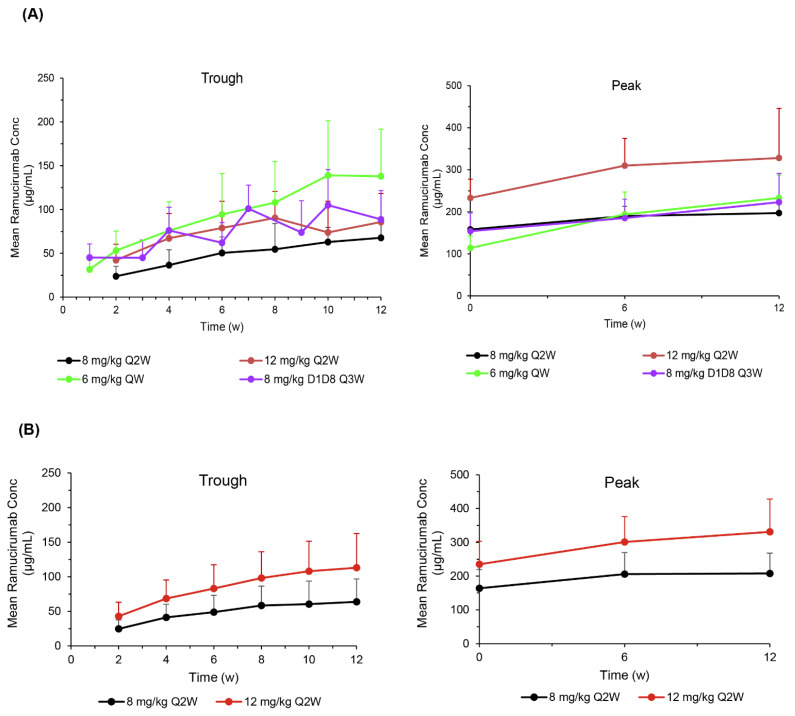
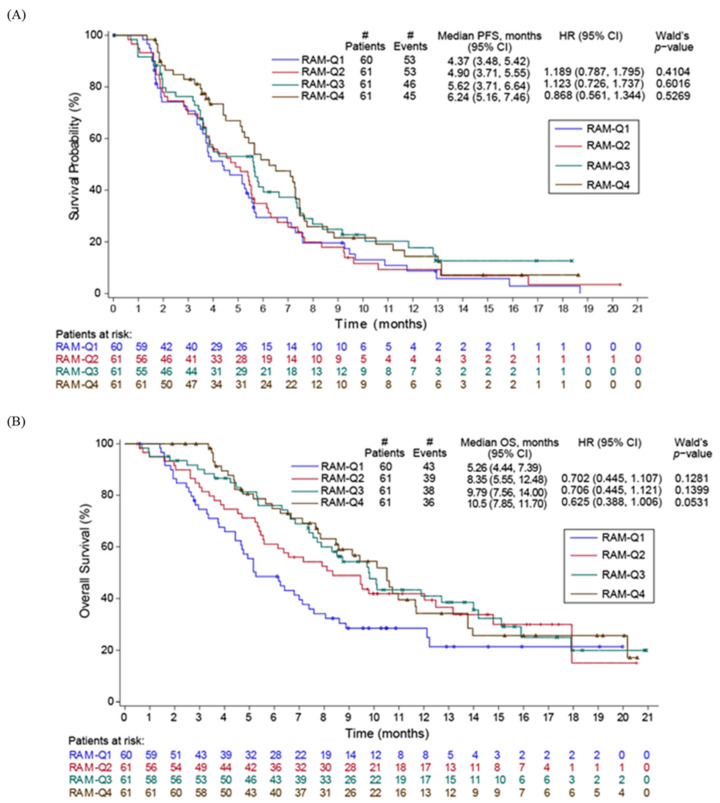
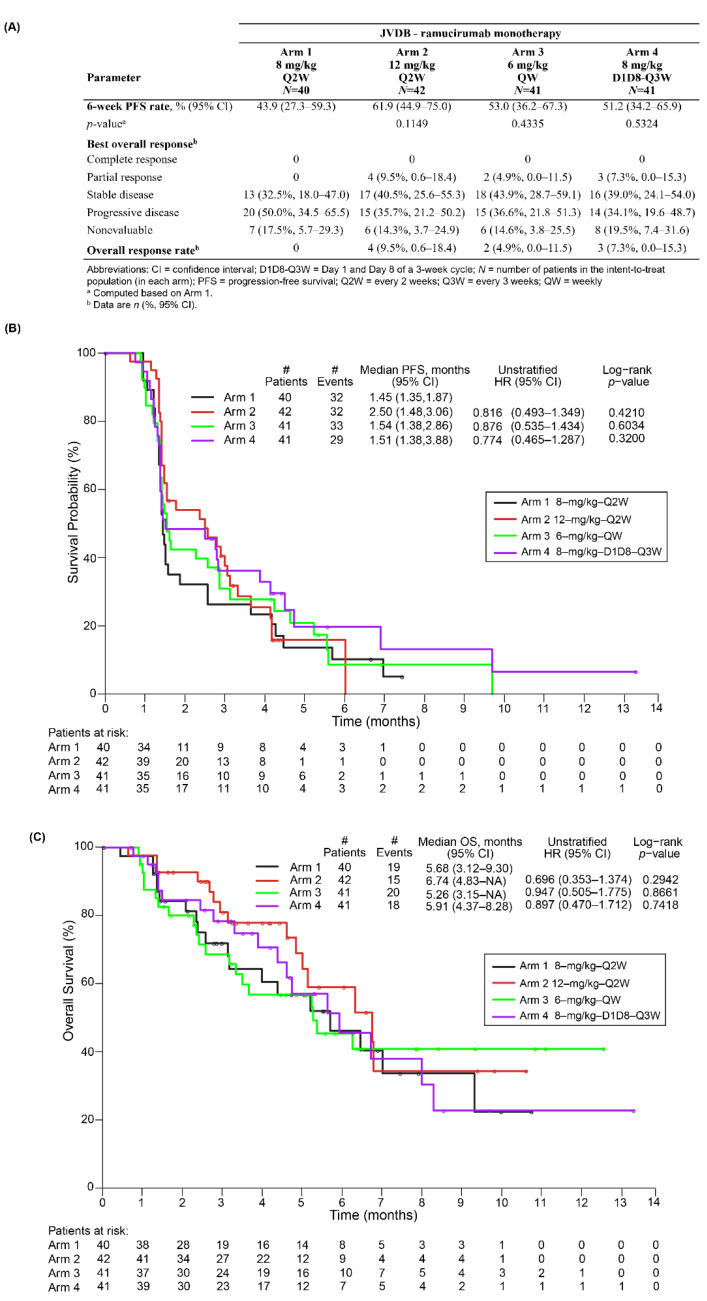
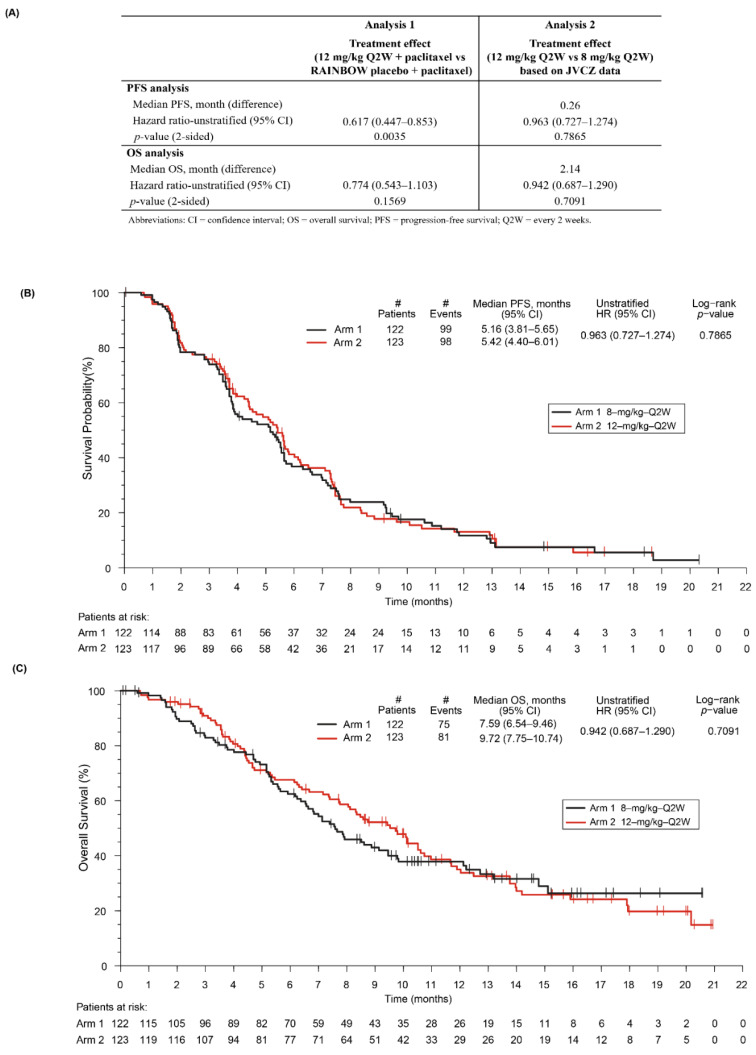
Studies JVDB and JVCZ examined alternative ramucirumab dosing regimens as monotherapy or combined with paclitaxel, respectively, in patients with advanced/metastatic gastric/gastroesophageal junction (GEJ) adenocarcinoma. For JVDB, randomized patients ( = 164) received ramucirumab monotherapy at four doses: 8 mg/kg every 2 weeks (Q2W) (registered dose), 12 mg/kg Q2W, 6 mg/kg weekly (QW), or 8 mg/kg on days 1 and 8 (D1D8) every 3 weeks (Q3W). The primary objectives were the safety and pharmacokinetics of ramucirumab monotherapy. For JVCZ, randomized patients ( = 245) received paclitaxel (80 mg/m-D1D8D15) plus ramucirumab (8 mg/kg- or 12 mg/kg-Q2W). The primary objective was progression-free survival (PFS) of 12 mg/kg-Q2W arm versus placebo from RAINBOW using meta-analysis. Relative to the registered dose, exploratory dosing regimens (EDRs) led to higher ramucirumab serum concentrations in both studies. EDR safety profiles were consistent with previous studies. In JVDB, serious adverse events occurred more frequently in the 8 mg/kg-D1D8-Q3W arm versus the registered dose; 6 mg/kg-QW EDR had a higher incidence of bleeding/hemorrhage. In JVCZ, PFS was improved with the 12 mg/kg plus paclitaxel combination versus placebo in RAINBOW; however, no significant PFS improvement was observed between the 12 mg/kg and 8 mg/kg arms. The lack of a dose/exposure-response relationship in these studies supports the standard dose of ramucirumab 8 mg/kg-Q2W as monotherapy or in combination with paclitaxel as second-line treatment for advanced/metastatic gastric/GEJ adenocarcinoma.
研究JVDB和JVCZ分别在晚期/转移性胃/胃食管交界(GEJ)腺癌患者中研究了雷莫西尤单抗作为单药治疗或与紫杉醇联合使用的替代给药方案。对于JVDB,随机分组的患者(n = 164)接受四种剂量的雷莫西尤单抗单药治疗:每2周一次(Q2W)8 mg/kg(注册剂量)、每2周一次12 mg/kg、每周一次(QW)6 mg/kg或每3周一次(Q3W)第1天和第8天(D1D8)8 mg/kg。主要目标是雷莫西尤单抗单药治疗的安全性和药代动力学。对于JVCZ,随机分组的患者(n = 245)接受紫杉醇(80 mg/m² - D1D8D15)加雷莫西尤单抗(8 mg/kg - 或12 mg/kg - Q2W)。主要目标是使用荟萃分析比较RAINBOW研究中12 mg/kg - Q2W组与安慰剂组的无进展生存期(PFS)。相对于注册剂量,探索性给药方案(EDR)在两项研究中均导致更高的雷莫西尤单抗血清浓度。EDR的安全性概况与先前研究一致。在JVDB中,8 mg/kg - D1D8 - QW组与注册剂量组相比,严重不良事件发生频率更高;6 mg/kg - QW EDR的出血/大出血发生率更高。在JVCZ中,RAINBOW研究中12 mg/kg加紫杉醇联合治疗组与安慰剂组相比PFS有所改善;然而,12 mg/kg组和8 mg/kg组之间未观察到PFS有显著改善这些研究中缺乏剂量/暴露 - 反应关系支持雷莫西尤单抗8 mg/kg - Q2W作为单药治疗或与紫杉醇联合作为晚期/转移性胃/GEJ腺癌二线治疗的标准剂量。