Department of Endocrinology, University Hospitals of Leicester NHS Trust, Leicester Royal Infirmary, Leicester, UK.
Clin Endocrinol (Oxf). 2022 Nov;97(5):643-653. doi: 10.1111/cen.14721. Epub 2022 Mar 20.
To investigate the long-term outcomes and prognosis of thyrotoxicosis in a large number of patients in a single UK county (Leicestershire).
Retrospective cohort analysis of 56,741 thyroid function test (TFT) results, treatment modalities and outcomes in a well-established virtual thyrotoxicosis clinic database.
One thousand four hundred and eighty-nine patients were included with a median length of follow-up of 10.9 years. The aetiology of thyrotoxicosis was autoimmune (85.9%), nodular (9.1%) and mixed (5.0%). Treatment modalities included antithyroid drugs (ATDs), radioiodine (RAI; 555 MBq fixed dose) and thyroidectomy.
We analysed both individual TFTs and groups of sequential TFTs on or after the same thyroid treatment(s), which we describe as 'phase of thyroid care' (POTC). Patients studied entered the virtual clinic between 1 January 1995 and 1 January 2010; we exported data on every TFT sample up to April 2020.
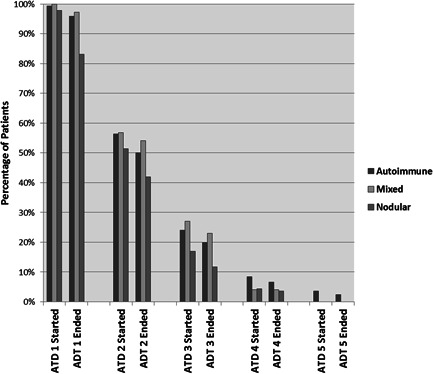
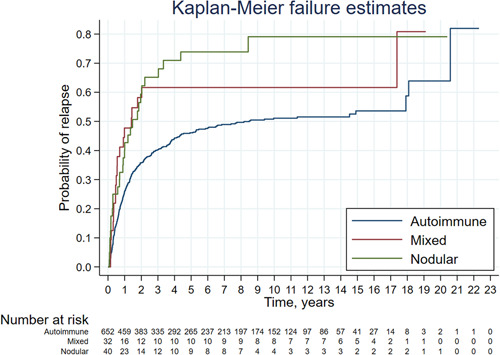
ATD had been used in 99.2% (median 2, maximum seven courses) with long-term ATD (>2 years) in 48%. RAI and thyroidectomy were used more commonly with nodular and mixed aetiology. Overall, T4 was more often controlled than thyroid-stimulating hormone (TSH), and at the latest follow-up, T4 was normal in >96%, TSH in >79% and both in >76% of different aetiologies. The mean percentage control of T4 was 85% and TSH 50%; in long-term ATD courses, this improved to 89% and 62%, respectively. In the latest POTC, control of T4 and TSH was best in cases off treatment (95%/87%) and on T4 without ablative therapy (94%/72%), but was broadly similar in patients on long-term ATD (90%/68%), after RAI (92%/60%) or after thyroidectomy (91%/58%). After the first course of ATD, remission or hypothyroidism was seen in 47.3% autoimmune, 20.9% nodular and 32.5% mixed, with 90% relapses seen within 4 years. Relapse was more common in patients with ophthalmopathy, but there was no difference between the sexes.
Thyrotoxicosis can be well controlled with minimal specialist clinic attendance using a software-supported virtual shared-care scheme. Long-term ATD appears to be a valid patient choice achieving TFT control comparable to that seen after RAI or surgery. In patients with autoimmune disease, relapse is more common in patients with ophthalmopathy, and hypothyroidism is common after RAI. In nodular disease, we found that spontaneous remission may occur.
在英国莱斯特郡的一个大型单一县(莱斯特郡)中,调查大量甲状腺功能亢进症患者的长期结果和预后。
在一个成熟的虚拟甲状腺功能亢进症诊所数据库中,对 56741 次甲状腺功能检测(TFT)结果、治疗方式和结局进行回顾性队列分析。
共纳入 1489 例患者,中位随访时间为 10.9 年。甲状腺功能亢进症的病因是自身免疫性(85.9%)、结节性(9.1%)和混合性(5.0%)。治疗方法包括抗甲状腺药物(ATD)、放射性碘(RAI;555MBq 固定剂量)和甲状腺切除术。
我们分析了在相同甲状腺治疗后或之后的单个 TFT 和连续 TFT 组,我们将其描述为“甲状腺护理阶段(POTC)”。研究中的患者于 1995 年 1 月 1 日至 2010 年 1 月 1 日期间进入虚拟诊所;我们在 2020 年 4 月之前导出了每个 TFT 样本的数据。
ATD 的使用比例为 99.2%(中位数 2 次,最大 7 次疗程),长期 ATD(>2 年)的使用比例为 48%。RAI 和甲状腺切除术在结节性和混合性病因中更为常见。总的来说,T4 的控制比甲状腺刺激激素(TSH)更为常见,在最新的随访中,不同病因中 T4 正常的比例>96%,TSH 正常的比例>79%,两者均正常的比例>76%。T4 的平均控制百分比为 85%,TSH 为 50%;在长期 ATD 疗程中,分别改善至 89%和 62%。在最新的 POTC 中,在无治疗(95%/87%)和无消融治疗(94%/72%)时,T4 和 TSH 的控制最好,但在长期接受 ATD(90%/68%)、接受 RAI(92%/60%)或接受甲状腺切除术(91%/58%)的患者中,情况大致相似。在接受第一疗程 ATD 后,自身免疫性甲状腺功能亢进症患者中缓解或甲状腺功能减退的比例为 47.3%,结节性甲状腺功能亢进症患者为 20.9%,混合性甲状腺功能亢进症患者为 32.5%,90%的患者在 4 年内出现复发。眼病患者复发更为常见,但男女之间无差异。
使用支持软件的虚拟共享护理方案,甲状腺功能亢进症可以得到很好的控制,只需很少的专科门诊就诊。长期 ATD 似乎是一种有效的患者选择,可以实现与 RAI 或手术相似的 TFT 控制。在自身免疫性疾病患者中,眼病患者更常见复发,RAI 后甲状腺功能减退症常见。在结节性疾病中,我们发现自发缓解可能发生。