Early Cancer Institute, Department of Oncology, University of Cambridge, Cambridge, UK.
Department of Gastroenterology, Hepatology and Clinical Oncology, Centre of Postgraduate Medical Education, Warsaw, Poland.
Histopathology. 2022 Jun;80(7):1081-1090. doi: 10.1111/his.14642.
Barrett's oesophagus with indefinite for dysplasia (BE-IND) is a subjective diagnosis with a low interobserver agreement (IOA) among pathologists and uncertain clinical implications. This study aimed to assess the utility of p53 immunohistochemistry (p53-IHC) in assessing BE-IND specimens.
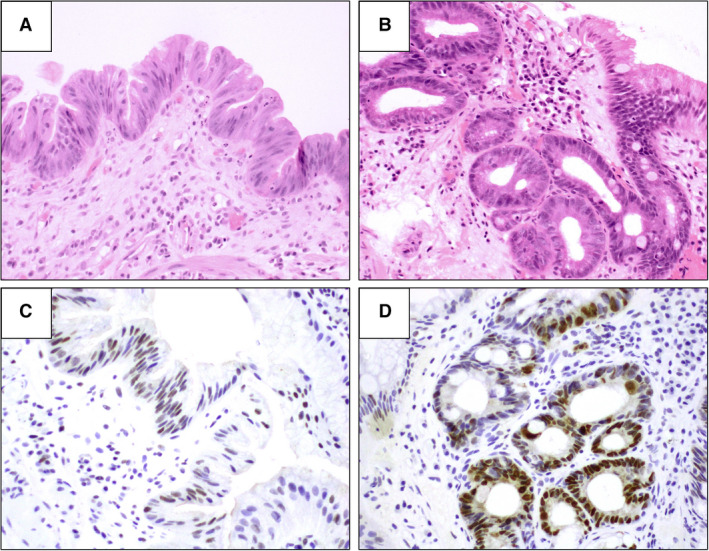
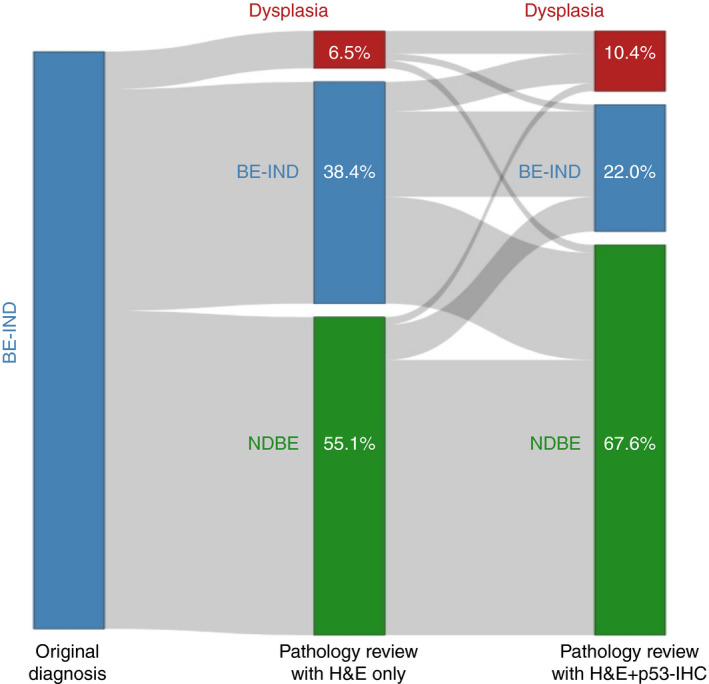
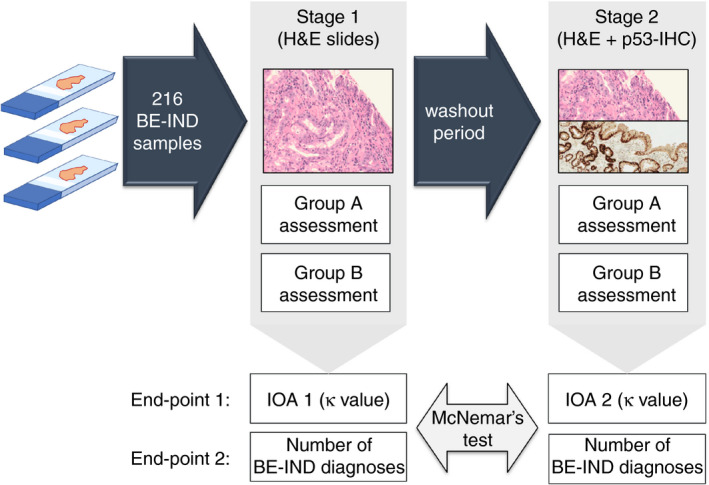
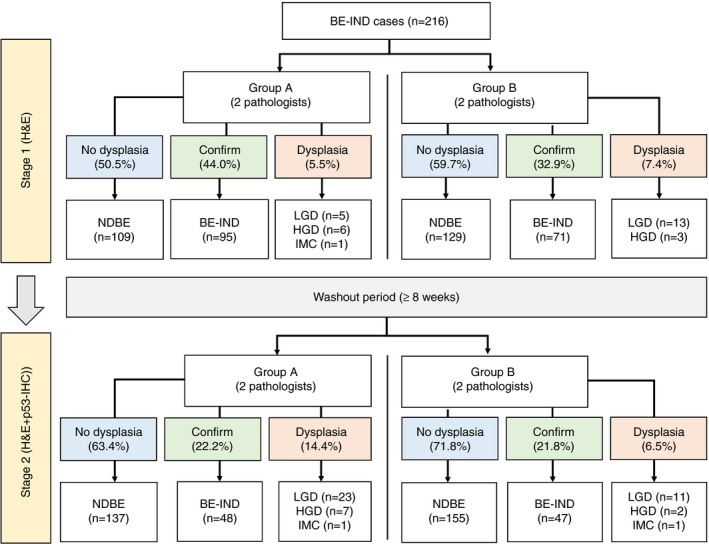
Archive endoscopic biopsies with a BE-IND diagnosis from two academic centres were analysed. First, haematoxylin and eosin-stained slides (H&E) were reviewed by four expert gastrointestinal (GI) pathologists allocated into two groups (A and B). After a washout period of at least 8 weeks, H&E slides were reassessed side-to-side with p53-IHC available. We compared the rate of changed diagnosis and the IOA for all BE grades before and after p53-IHC. We included 216 BE-IND specimens from 185 patients, 44.0 and 32.9% of which were confirmed after H&E slide revision by groups A and B, respectively. More than half the cases were reclassified to a non-dysplastic BE (NDBE), while 5.6% of cases in group A and 7.4% in group B were reclassified to definite dysplasia. The IOA for NDBE, BE-IND, low-grade dysplasia (LGD) and high-grade dysplasia (HGD)/intramucosal cancer (IMC) was 0.31, 0.21, -0.03 and -0.02, respectively. Use of p53-IHC led to a >40% reduction in BE-IND diagnoses (P < 0.001) and increased IOA for all BE grades [κ = 0.46 (NDBE), 0.26 (BE-IND), 0.49 (LGD), 0.35 (HGD/IMC)]. An aberrant p53-IHC pattern significantly increased the likelihood of reclassifying BE-IND to definite dysplasia (odds ratio = 44.3, 95% confidence interval = 18.8-113.0).
P53-IHC reduces the rate of BE-IND diagnoses and improves the IOA among pathologists when reporting BE with equivocal epithelial changes.
巴雷特食管伴不确定异型增生(BE-IND)是一种主观诊断,病理学家之间的观察者间一致性(IOA)较低,且临床意义不确定。本研究旨在评估 p53 免疫组化(p53-IHC)在评估 BE-IND 标本中的作用。
分析了来自两个学术中心的具有 BE-IND 诊断的存档内镜活检。首先,由四位分配到两组(A 和 B)的专家胃肠病学(GI)病理学家对苏木精和伊红染色(H&E)幻灯片进行了回顾。经过至少 8 周的洗脱期后,可用 p53-IHC 对 H&E 幻灯片进行侧对侧评估。我们比较了所有 BE 分级在 p53-IHC 前后改变诊断的比率和 IOA。我们纳入了来自 185 名患者的 216 例 BE-IND 标本,A 组和 B 组分别通过 H&E 幻灯片修订后确认了 44.0%和 32.9%的病例。超过一半的病例被重新分类为非异型增生性 BE(NDBE),而 A 组的 5.6%和 B 组的 7.4%的病例被重新分类为明确异型增生。NDBE、BE-IND、低级别异型增生(LGD)和高级别异型增生(HGD)/黏膜内癌(IMC)的 IOA 分别为 0.31、0.21、-0.03 和-0.02。使用 p53-IHC 导致 BE-IND 诊断减少了>40%(P<0.001),并增加了所有 BE 分级的 IOA[κ=0.46(NDBE)、0.26(BE-IND)、0.49(LGD)、0.35(HGD/IMC)]。异常的 p53-IHC 模式显著增加了将 BE-IND 重新分类为明确异型增生的可能性(比值比=44.3,95%置信区间=18.8-113.0)。
当报告具有不确定上皮变化的 BE 时,p53-IHC 可降低 BE-IND 诊断的发生率,并提高病理学家之间的 IOA。