MRC Cancer Unit, University of Cambridge, Hutchison/MRC Research Centre, Box 197, Cambridge Biomedical Campus, Cambridge CB2 0XZ, United Kingdom.
Department of Gastroenterology, Amsterdam University Medical Centre, Meibergdreef 9, 1105 AZ, Amsterdam 22660, the Netherlands.
EBioMedicine. 2020 Jun;56:102765. doi: 10.1016/j.ebiom.2020.102765. Epub 2020 May 24.
The cancer risk in Barrett's oesophagus (BO) is difficult to estimate. Histologic dysplasia has strong predictive power, but can be missed by random biopsies. Other clinical parameters have limited utility for risk stratification. We aimed to assess whether a molecular biomarker panel on targeted biopsies can predict neoplastic progression of BO.
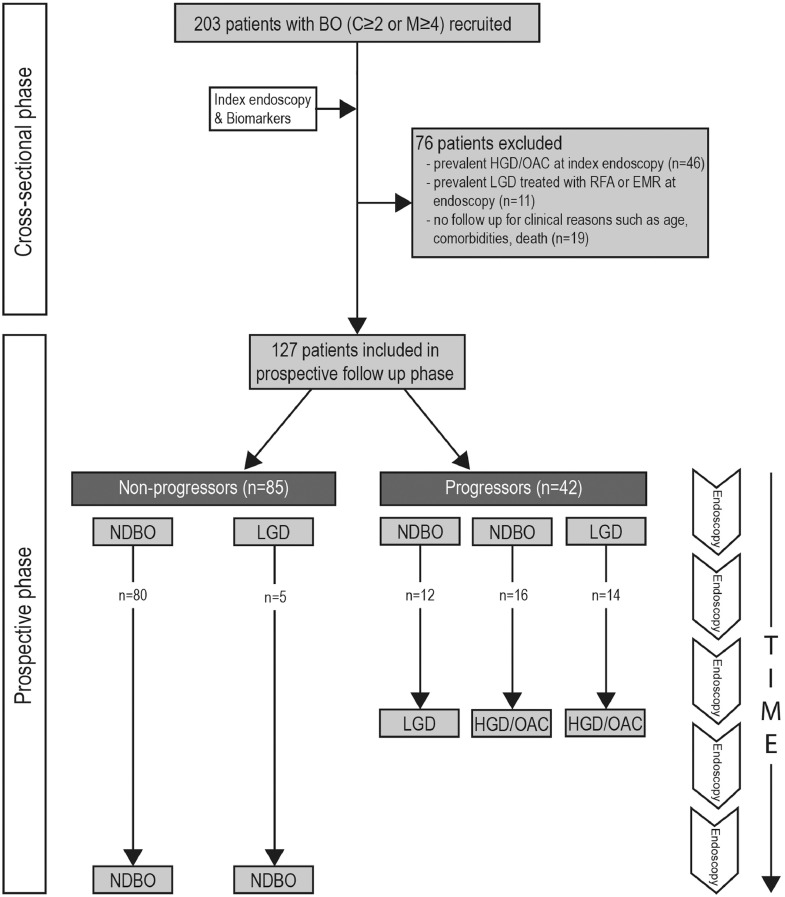
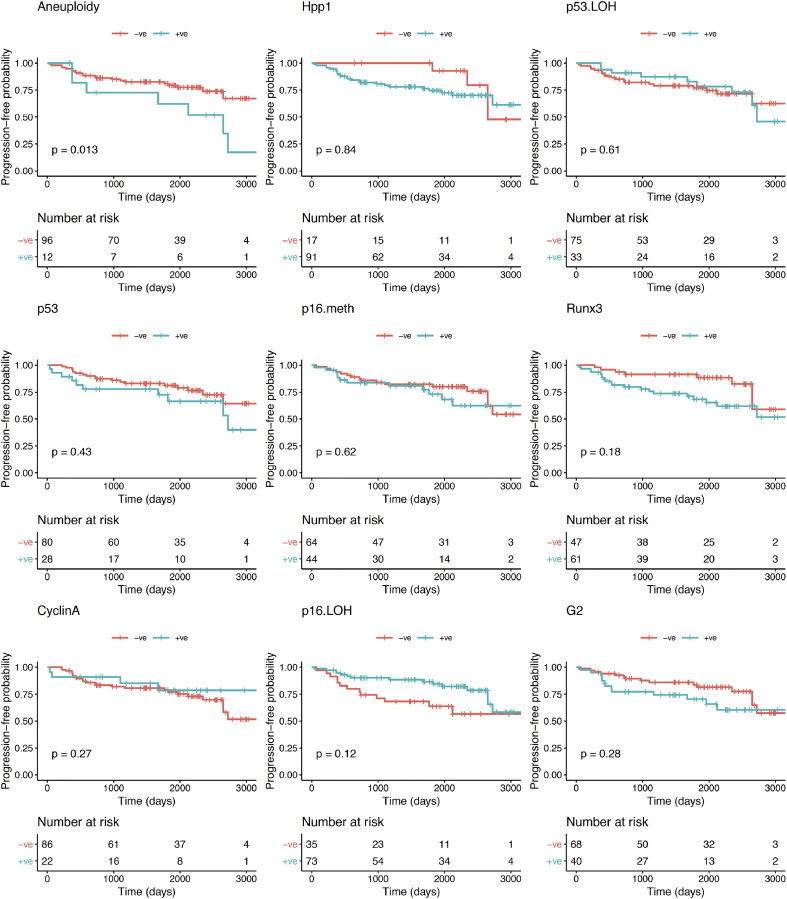
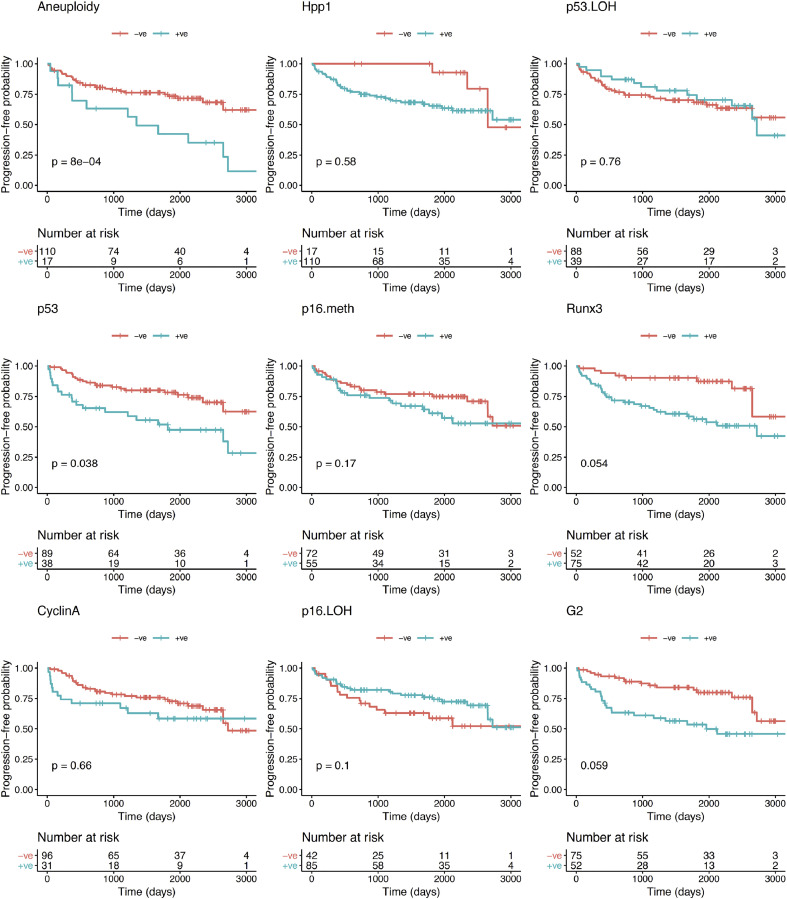
203 patients with BO were tested at index endoscopy for 9 biomarkers (p53 and cyclin A expression; aneuploidy and tetraploidy; CDKN2A (p16), RUNX3 and HPP1 hypermethylation; 9p and 17p loss of heterozygosity) on autofluorescence-targeted biopsies and followed-up prospectively. Data comparing progressors to non-progressors were evaluated by univariate and multivariate analyses using survival curves, Cox-proportional hazards and logistic regression models.
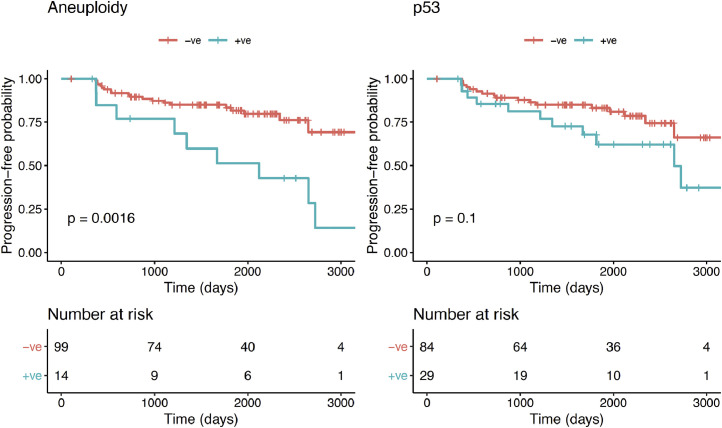
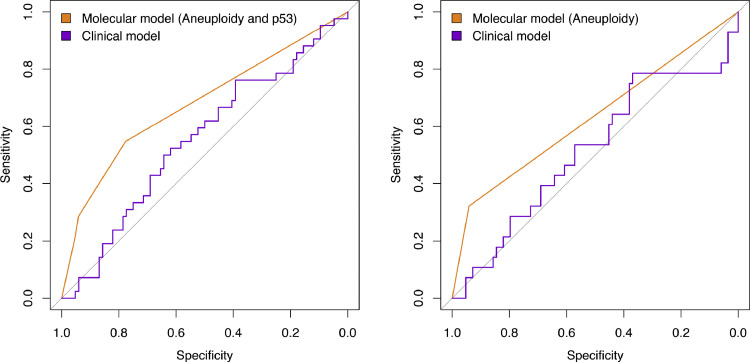
127 patients without high-grade dysplasia (HGD) or oesophageal adenocarcinoma (OAC) at index endoscopy were included, of which 42 had evidence of any histologic progression over time. Aneuploidy was the only predictor of progression from non-dysplastic BO (NDBO) to any grade of neoplasia (p = 0.013) and HGD/OAC (p = 0.002). Aberrant p53 expression correlated with risk of short-term progression within 12 months, with an odds ratio of 6.0 (95% CI: 3.1-11.2). A panel comprising aneuploidy and p53 had an area under the receiving operator characteristics curve of 0.68 (95% CI: 0.59-0.77) for prediction of any progression.
Aneuploidy is the only biomarker that predicts neoplastic progression of NDBO. Aberrant p53 expression suggests prevalent dysplasia, which might have been missed by random biopsies, and warrants early follow up.
巴雷特食管(BO)的癌症风险难以估计。组织学异型增生具有很强的预测能力,但可能会被随机活检遗漏。其他临床参数对风险分层的实用性有限。我们旨在评估靶向活检的分子生物标志物是否可以预测 BO 的肿瘤进展。
203 名 BO 患者在首次内镜检查时接受了 9 种生物标志物(p53 和细胞周期蛋白 A 表达;非整倍体和四倍体;CDKN2A(p16)、RUNX3 和 HPP1 高甲基化;9p 和 17p 杂合性丢失)的检测,采用自动荧光靶向活检,并进行前瞻性随访。使用生存曲线、Cox 比例风险和逻辑回归模型对进展者和非进展者的数据进行单变量和多变量分析。
共有 127 名在首次内镜检查时无高级别异型增生(HGD)或食管腺癌(OAC)的患者被纳入研究,其中 42 名患者在随访过程中存在任何程度的组织学进展。非整倍体是从非异型增生性 BO(NDBO)进展为任何程度肿瘤(p=0.013)和 HGD/OAC(p=0.002)的唯一预测因素。异常的 p53 表达与 12 个月内短期进展的风险相关,优势比为 6.0(95%CI:3.1-11.2)。包含非整倍体和 p53 的生物标志物组合预测任何进展的接收者操作特征曲线下面积为 0.68(95%CI:0.59-0.77)。
非整倍体是唯一能预测 NDBO 肿瘤进展的生物标志物。异常的 p53 表达提示普遍存在异型增生,这可能被随机活检遗漏,需要早期随访。