Tongyoo Surat, Chanthawatthanarak Sivit, Permpikul Chairat, Ratanarat Ranistha, Promsin Panuwat, Kongsayreepong Suneerat
Division of Critical Care, Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand.
Department of Emergency Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand.
J Thorac Dis. 2022 Feb;14(2):371-380. doi: 10.21037/jtd-21-1460.
Extracorporeal membrane oxygenation (ECMO) is an important rescue therapy for patients with refractory respiratory or circulatory failure. High cost and associated complications warrant careful case selection. The aim of this study was to investigate the outcomes and factors associated with mortality in acute hypoxemic respiratory failure patients who received ECMO support, and to externally validate preexisting ECMO survival prediction scoring systems.
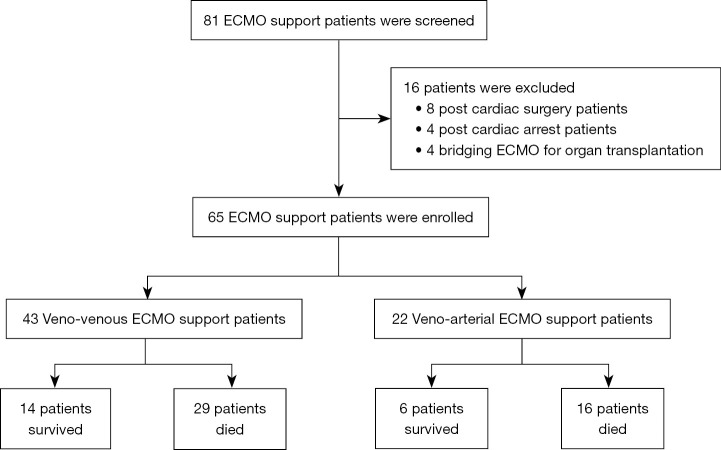
This retrospective study enrolled acute hypoxemic respiratory failure patients who received veno-venous (VV) or veno-arterial (VA) ECMO support at Siriraj Hospital (Bangkok, Thailand) from 2010 to 2020. All relevant baseline patient characteristics including ECMO survival prediction scores were recorded. The primary outcome was in-hospital mortality. Multivariate logistic regression analysis was employed to identify independent predictors of in-hospital mortality.
Of a total of 65 patients, 34 (52%) were male, the median (IQR) age was 61 years (49-70 years), the median body mass index (BMI) was 22.6 kg/m (20.6-28 kg/m), and the median Sequential Organ Failure Assessment (SOFA) score was 13 [11-16]. Forty-three patients (66%) received VV-ECMO, and 22 (34%) received VA-ECMO support. In-hospital mortality was 69%. Multivariate analysis identified a SOFA score >14, hospitalized >72 hours before ECMO initiation, PaO/FiO ratio <60, and pH <7.2 as independent predictors of in-hospital mortality. These four parameters were combined to create the SHOP (S: SOFA >14, H: hospitalize >72 hours, O: PF ratio <60, and P: pH <7.2) score. Compared with three different preexisting ECMO survival prediction scoring systems, the SHOP score had the highest area under the curve (AUC) for predicting in-hospital mortality (overall: 0.873, VV-EMCO: 0.866, and VA-EMCO: 0.891).
In-hospital mortality among ECMO-supported patients was high at 69%. SOFA score >14, hospitalized >72 hours, PaO/FiO ratio <60, and pH <7.2 were found to be independent predictors of in-hospital mortality. A SHOP score of 2 or higher significantly predicts in-hospital mortality in EMCO-supported patients.
www.clinicaltrials.gov (reg. No. NCT04031794).
体外膜肺氧合(ECMO)是治疗难治性呼吸或循环衰竭患者的重要抢救疗法。高昂的费用和相关并发症使得病例选择需谨慎。本研究旨在调查接受ECMO支持的急性低氧性呼吸衰竭患者的预后及与死亡率相关的因素,并对外验证现有的ECMO生存预测评分系统。
这项回顾性研究纳入了2010年至2020年在泰国曼谷诗里拉吉医院接受静脉-静脉(VV)或静脉-动脉(VA)ECMO支持的急性低氧性呼吸衰竭患者。记录了所有相关的患者基线特征,包括ECMO生存预测评分。主要结局是院内死亡率。采用多因素逻辑回归分析确定院内死亡率的独立预测因素。
总共65例患者中,34例(52%)为男性,年龄中位数(IQR)为61岁(49 - 70岁),体重指数(BMI)中位数为22.6 kg/m²(20.6 - 28 kg/m²),序贯器官衰竭评估(SOFA)评分中位数为13[11 - 16]。43例患者(66%)接受VV-ECMO,22例(34%)接受VA-ECMO支持。院内死亡率为69%。多因素分析确定SOFA评分>14、在开始ECMO前住院>72小时、动脉血氧分压/吸入氧浓度(PaO₂/FiO₂)比值<60以及pH<7.2是院内死亡率的独立预测因素。将这四个参数组合创建了SHOP(S:SOFA>14,H:住院>72小时,O:PF比值<60,P:pH<7.2)评分。与三种现有的ECMO生存预测评分系统相比,SHOP评分在预测院内死亡率方面曲线下面积(AUC)最高(总体:0.873,VV-EMCO:0.866,VA-EMCO:0.891)。
接受ECMO支持的患者院内死亡率高达69%。发现SOFA评分>14、住院>72小时、PaO₂/FiO₂比值<60以及pH<7.2是院内死亡率的独立预测因素。SHOP评分为2分或更高显著预测接受EMCO支持患者的院内死亡率。