van Nunen Sheryl A, Burk Melanie B, Burton Pamela K, Ford Geoffrey, Harvey Richard J, Lozynsky Alexander, Pickford Elizabeth, Rimmer Janet S, Smart Joanne, Sutherland Michael F, Thien Francis, Weber Heinrich C, Zehnwirth Harry, Newbigin Ed, Katelaris Constance H
Northern Clinical School, Sydney Medical School, Faculty of Medicine and Health, The University of Sydney, Sydney, Australia.
Department of Clinical Immunology and Allergy, Royal North Shore Hospital, Sydney, Australia.
World Allergy Organ J. 2022 Feb 23;15(2):100632. doi: 10.1016/j.waojou.2022.100632. eCollection 2022 Feb.
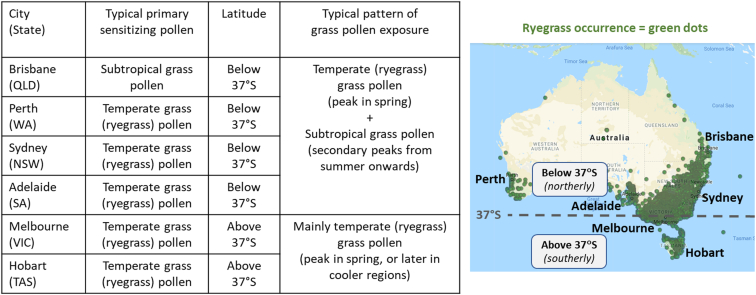
Temperate grass (eg, ryegrass) pollen is a major driver of seasonal allergic rhinitis (SAR) and asthma risks, including thunderstorm asthma. Data for the effectiveness of temperate grass pollen allergen immunotherapy (AIT) in SAR patients from the southern hemisphere, who are frequently polysensitized to subtropical grass pollens, are limited. The 300 IR 5-grass pollen sublingual immunotherapy tablet (300 IR 5-grass SLIT) is known to be effective in polysensitized SAR patients with primary allergy to temperate grasses, however, the influence of polysensitization to subtropical grass pollen on treatment responses has yet to be specifically addressed. Key aims of this study were to measure patient treatment satisfaction during 300 IR 5-grass SLIT treatment and evaluate how polysensitization to subtropical grass pollens affects treatment responses.
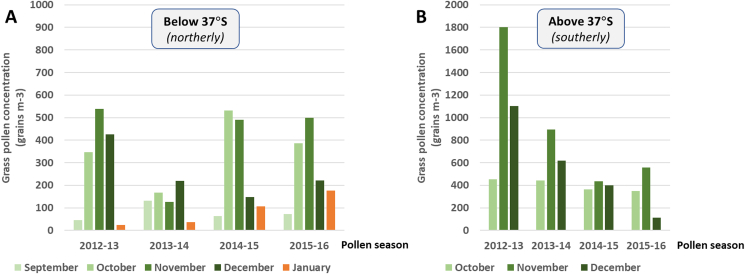
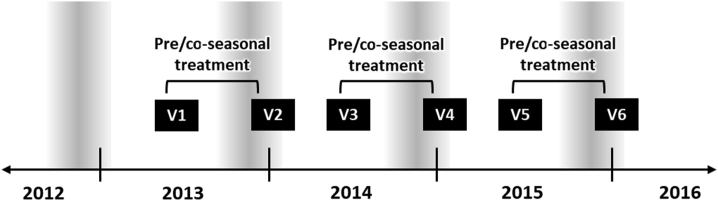
A prospective observational study was conducted in 63 patients (aged ≥5 years) in several temperate regions of Australia prescribed 300 IR 5-grass SLIT for SAR over 3 consecutive grass pollen seasons. Ambient levels of pollen were measured at representative sites. Patient treatment satisfaction was assessed using a QUARTIS questionnaire. Rhinoconjunctivitis Total Symptom Score (RTSS) and a Hodges-Lehmann Estimator analysis was performed to evaluate if polysensitization to subtropical grass pollen affected SAR symptom intensity changes during SLIT.
A diagnosis of ryegrass pollen allergy was nearly universal. There were 74.6% (47/63) polysensitized to subtropical and temperate grass pollens. There were 23.8% (15/63) monosensitized to temperate grass pollens. From the first pollen season, statistically significant improvements occurred in SAR symptoms compared with baseline in both monosensitized and polysensitized patients, particularly in those polysensitized (P = 0.0297). Improvements in SAR symptoms were sustained and similar in both groups in the second and third pollen seasons, reaching 70-85% improvement (P < 0.01). Polysensitized patients from both northerly and southerly temperate regions in Australia showed similar improvements. Grass pollen counts in both regions were consistently highest during springtime.
300 IR 5-grass SLIT is effective in a real-life setting in SAR patients in the southern hemisphere with primary allergy to temperate grass pollen and predominantly springtime grass pollen exposures. Importantly, SLIT treatment effectiveness was irrespective of the patient's polysensitization status to subtropical grass pollens.
温带草(如黑麦草)花粉是季节性过敏性鼻炎(SAR)和哮喘风险(包括雷暴哮喘)的主要驱动因素。来自南半球的SAR患者对亚热带草花粉常常多敏,关于温带草花粉变应原免疫疗法(AIT)对这类患者有效性的数据有限。已知300 IR 5 -草花粉舌下免疫疗法片剂(300 IR 5 -草SLIT)对原发性温带草过敏的多敏SAR患者有效,然而,对亚热带草花粉的多敏状态对治疗反应的影响尚未得到具体研究。本研究的主要目的是测量300 IR 5 -草SLIT治疗期间患者的治疗满意度,并评估对亚热带草花粉的多敏状态如何影响治疗反应。
在澳大利亚几个温带地区对63例年龄≥5岁的患者进行了一项前瞻性观察研究,这些患者在连续3个草花粉季节接受300 IR 5 -草SLIT治疗以治疗SAR。在代表性地点测量环境花粉水平。使用QUARTIS问卷评估患者的治疗满意度。进行鼻结膜炎总症状评分(RTSS)和霍奇斯 - Lehmann估计分析,以评估对亚热带草花粉的多敏状态是否影响SLIT期间SAR症状强度的变化。
几乎所有患者都被诊断为黑麦草花粉过敏。74.6%(47/63)的患者对亚热带和温带草花粉多敏。23.8%(15/63)的患者对温带草花粉单敏。从第一个花粉季节开始,单敏和多敏患者的SAR症状与基线相比均有统计学显著改善,尤其是多敏患者(P = 0.0297)。在第二个和第三个花粉季节,两组的SAR症状改善持续且相似,改善率达到70 - 85%(P < 0.01)。澳大利亚北部和南部温带地区的多敏患者表现出相似的改善。两个地区的草花粉计数在春季始终最高。
300 IR 5 -草SLIT在现实环境中对南半球原发性温带草花粉过敏且主要在春季接触草花粉的SAR患者有效。重要的是,SLIT治疗效果与患者对亚热带草花粉的多敏状态无关。