Taylor Douglas J, Halpern Vera, Brache Vivian, Bahamondes Luis, Jensen Jeffrey T, Dorflinger Laneta J
FHI 360, Durham, NC, United States.
Profamilia, Biomedical Research Department, Santo Domingo, Dominican Republic.
Contracept X. 2022 Feb 23;4:100073. doi: 10.1016/j.conx.2022.100073. eCollection 2022.
To characterize the relationship between serum medroxyprogesterone acetate (MPA) concentrations and ovulation suppression, and to estimate the risk of ovulation for investigational subcutaneous regimens of Depo-Provera CI (Depo-Provera) and Depo-subQ Provera 104 (Depo-subQ).
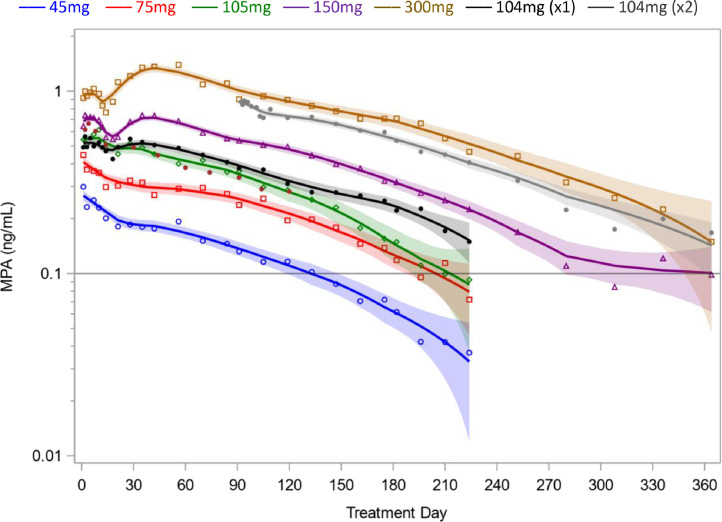
We performed a secondary analysis of 2 studies that assessed the pharmacokinetics and pharmacodynamics of MPA when Depo-Provera is administered subcutaneously rather than by the labeled intramuscular route. Each woman received a single 45 mg to 300 mg subcutaneous injection of Depo-Provera, a single 104 mg subcutaneous injection of Depo-subQ, or 2 injections of Depo-subQ at 3-month intervals. We used an elevation of serum progesterone ≥4.7 ng/mL as a surrogate for ovulation and non-parametric statistical methods to assess pharmacokinetic and pharmacodynamic relationships.
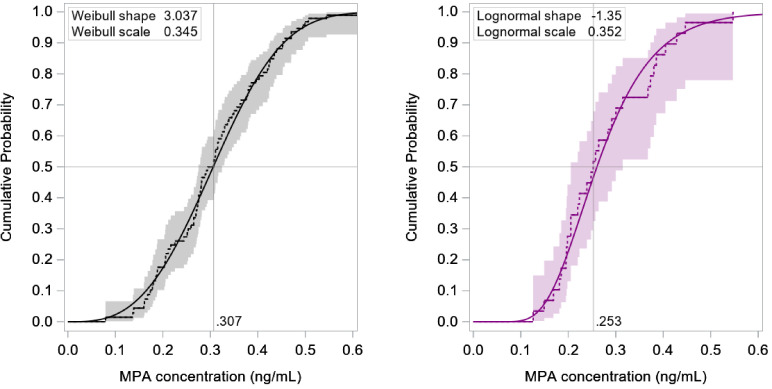
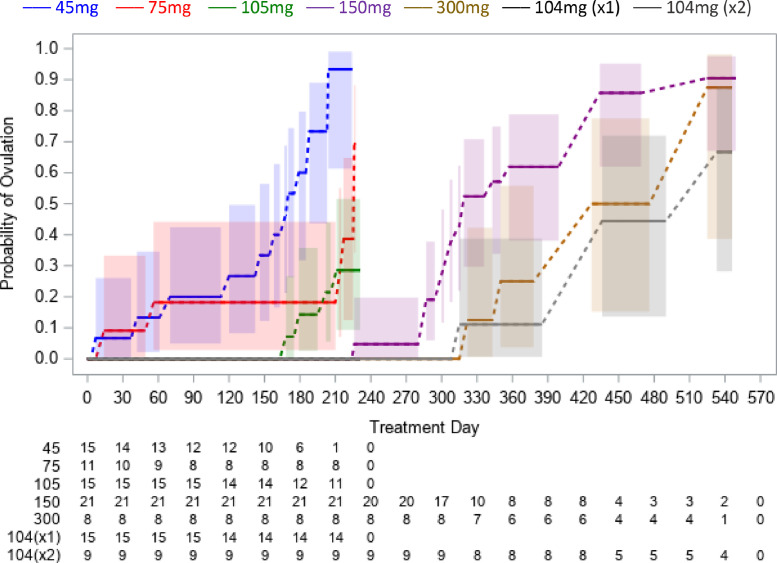
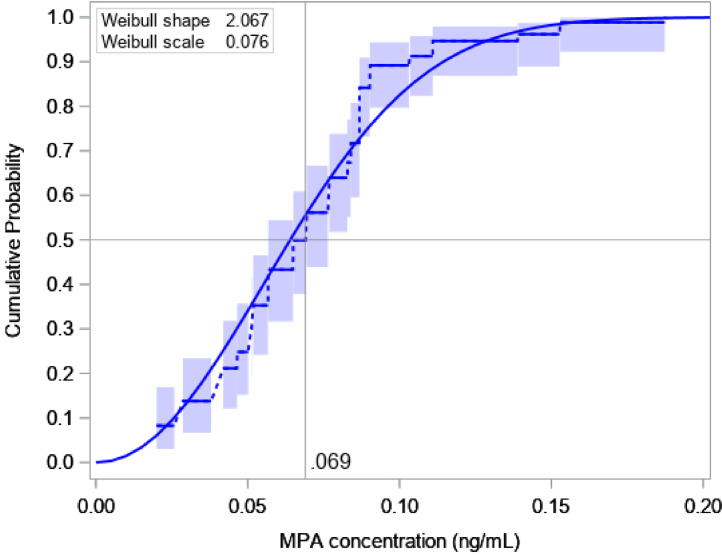
This analysis included 101 women with body mass index (BMI) 18 to 34 kg/m. Return of ovulation occurred at a median MPA concentration of 0.07 ng/mL (95% CI: 0.06-0.08) and the 90th percentile was 0.10 ng/mL (95% CI: 0.09-0.14). Neither age, race, nor BMI significantly influenced this relationship. The estimated probabilities of ovulation within 4 months of a 104 mg subcutaneous injection and within 7 months of a 150 mg subcutaneous injection (6 plus a 1-month grace) were each below 2.2%.
The typical MPA concentration associated with loss of ovulation suppression is substantially less than the commonly cited threshold of 0.2 ng/mL. Based on our results, MPA levels would rarely be low enough to permit ovulation if the Depo-subQ reinjection interval were extended to four months or if 150 mg Depo-Provera were injected subcutaneously every 6 months.
Extending the three-month Depo-subQ reinjection interval by one month would result in a 25% reduction in yearly MPA exposure, with little risk of pregnancy. Off-label subcutaneous administration of 150 mg Depo-Provera every 6 months would be a highly effective repurposing of an excellent product, with a similar reduction in cumulative exposure.
描述血清醋酸甲羟孕酮(MPA)浓度与排卵抑制之间的关系,并评估醋酸甲羟孕酮避孕针(Depo-Provera)和皮下注射用醋酸甲羟孕酮104(Depo-subQ)皮下注射研究方案的排卵风险。
我们对两项研究进行了二次分析,这两项研究评估了皮下注射而非标记的肌肉注射途径给予醋酸甲羟孕酮避孕针时MPA的药代动力学和药效学。每位女性接受一次45mg至300mg的醋酸甲羟孕酮避孕针皮下注射、一次104mg的皮下注射用醋酸甲羟孕酮104皮下注射,或每3个月间隔进行2次皮下注射用醋酸甲羟孕酮104注射。我们使用血清孕酮升高≥4.7ng/mL作为排卵的替代指标,并采用非参数统计方法评估药代动力学和药效学关系。
该分析纳入了101名体重指数(BMI)为18至34kg/m²的女性。排卵恢复发生时的MPA浓度中位数为0.07ng/mL(95%CI:0.06-0.08),第90百分位数为0.10ng/mL(95%CI:0.09-0.14)。年龄、种族和BMI均未对这种关系产生显著影响。104mg皮下注射后4个月内以及150mg皮下注射后7个月内(6个月加1个月宽限期)的排卵估计概率均低于2.2%。
与排卵抑制丧失相关的典型MPA浓度远低于通常引用的0.2ng/mL阈值。根据我们的结果,如果皮下注射用醋酸甲羟孕酮104的再注射间隔延长至4个月,或者每6个月皮下注射150mg醋酸甲羟孕酮避孕针,MPA水平很少会低到足以允许排卵。
将皮下注射用醋酸甲羟孕酮104的3个月再注射间隔延长1个月将使每年的MPA暴露量减少25%,怀孕风险很小。每6个月非标签皮下注射150mg醋酸甲羟孕酮避孕针将是一种优秀产品的高效重新利用,累积暴露量也会有类似减少。