Shaker Marcus S, Abrams Elissa M, Oppenheimer John, Singer Alexander G, Shaker Matthew, Fleck Daniel, Greenhawt Matthew, Grove Evan
Dartmouth Geisel School of Medicine, Hanover, NH, United States.
Department of Medicine, Dartmouth-Hitchcock Medical Center, Lebanon, NH, United States.
Front Cardiovasc Med. 2022 Feb 24;9:771679. doi: 10.3389/fcvm.2022.771679. eCollection 2022.
Sudden cardiac arrest (SCA) occurs in 0.4% of the general population and up to 6% or more of at-risk groups each year. Early CPR and defibrillation improves SCA outcomes but access to automatic external defibrillators (AEDs) remains limited.
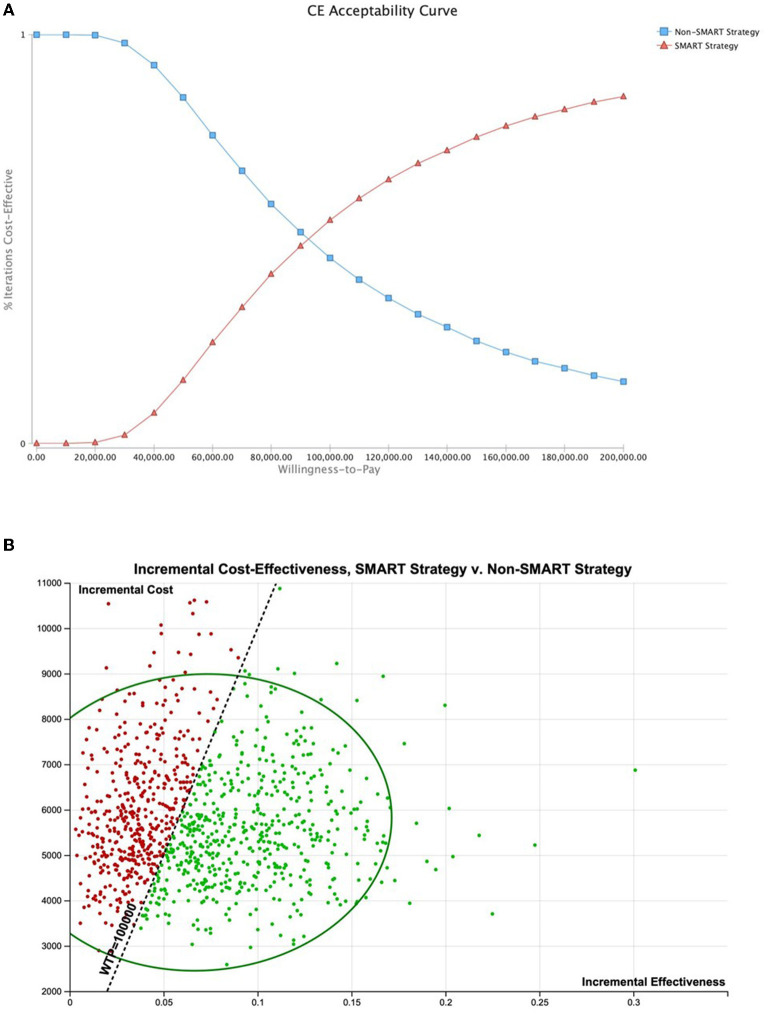
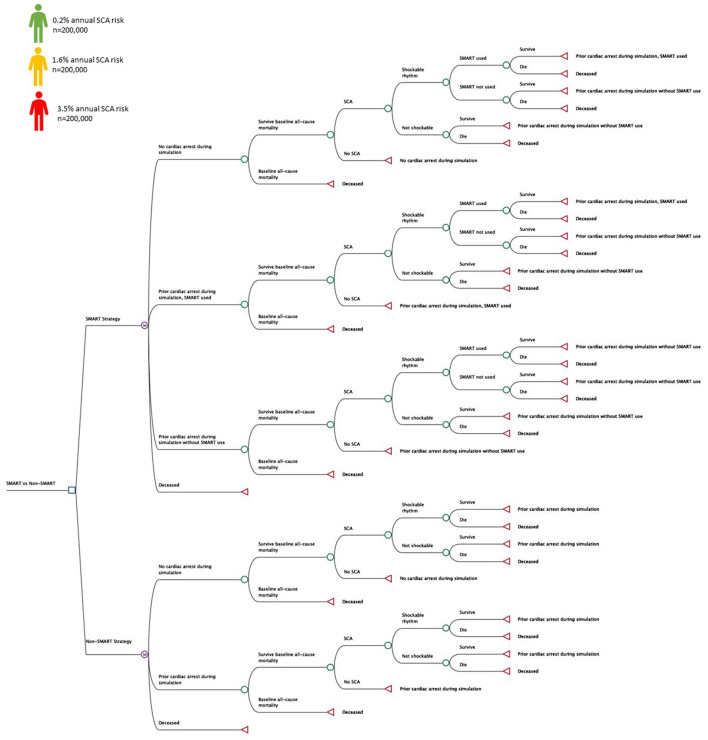
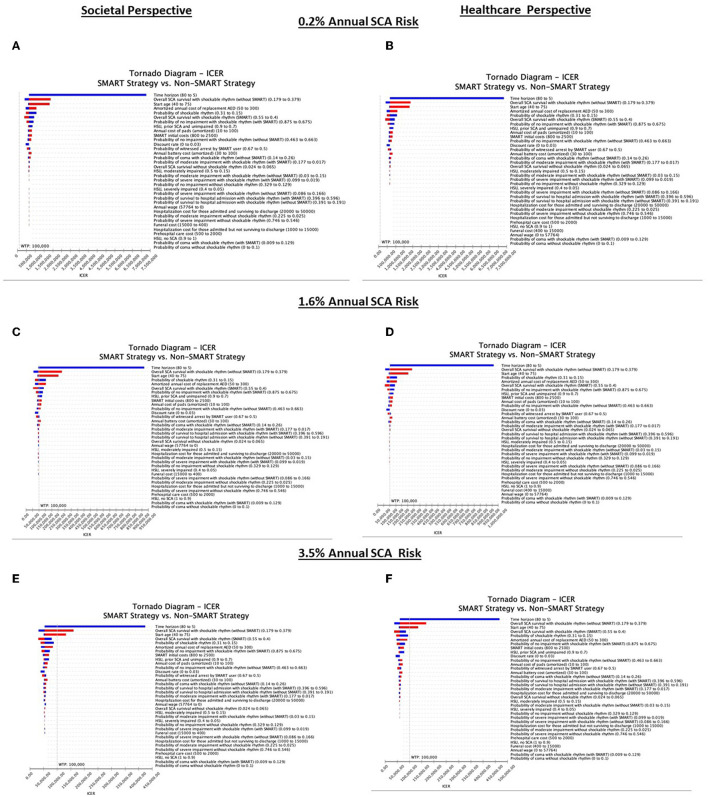
Markov models were used to evaluate the cost-effectiveness of a portable SMART (SMall AED for Rapid Treatment of SCA) approach to early SCA management over a life-time horizon in at-risk and not at-risk populations. Simulated patients ( = 600,000) who had not received an implantable cardioverter defibrillator (ICD) were randomized to a SMART device with CPR prompts or non-SMART approaches. Annual SCA risk was varied from 0.2 to 3.5%. Analysis was performed in a US economy from both societal (SP) and healthcare (HP) perspectives to evaluate the number of SCA fatalities prevented by SMART, and SMART cost-effectiveness at a threshold of $100,000/Quality Adjusted Life Year (QALY).
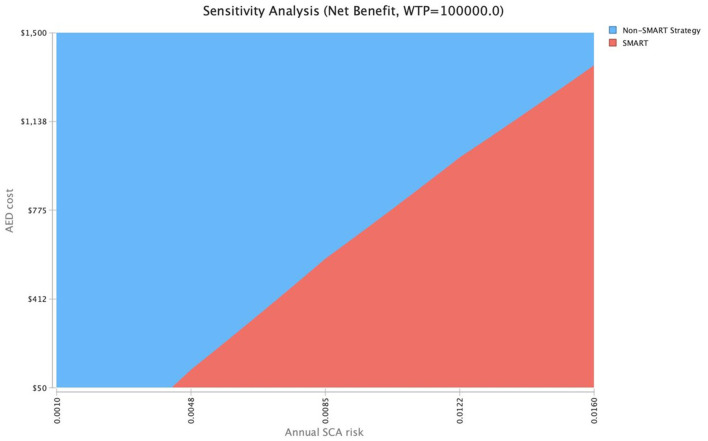
A SMART approach was cost-effective when annual SCA risk exceeded 1.51% (SP) and 1.62% (HP). The incremental cost-effectiveness ratios (ICER) were $95,251/QALY (SP) and $100,797/QALY (HP) at a 1.60% SCA annual risk. At a 3.5% annual SCA risk, SMART was highly cost-effective from both SP and HP [ICER: $53,925/QALY (SP), $59,672/QALY (HP)]. In microsimulation, SMART prevented 1,762 fatalities across risk strata (1.59% fatality relative risk reduction across groups). From a population perspective, SMART could prevent at least 109,839 SCA deaths in persons 45 years and older in the United States.
A SMART approach to SCA prophylaxis prevents fatalities and is cost-effective in patients at elevated SCA risk. The availability of a smart-phone enabled pocket-sized AED with CPR prompts has the potential to greatly improve population health and economic outcomes.
心脏骤停(SCA)在普通人群中的发生率为每年0.4%,在高危人群中的发生率高达6%或更高。早期心肺复苏(CPR)和除颤可改善SCA的治疗效果,但自动体外除颤器(AED)的可及性仍然有限。
采用马尔可夫模型,在高危和非高危人群的一生中,评估便携式SMART(用于快速治疗SCA的小型AED)方法对早期SCA管理的成本效益。将600,000名未接受植入式心脏复律除颤器(ICD)的模拟患者随机分为配备CPR提示的SMART设备组或非SMART方法组。年度SCA风险从0.2%变化到3.5%。从社会(SP)和医疗保健(HP)两个角度,在美国经济环境下进行分析,以评估SMART预防的SCA死亡人数,以及在100,000美元/质量调整生命年(QALY)的阈值下SMART的成本效益。
当年度SCA风险超过1.51%(SP)和1.62%(HP)时,SMART方法具有成本效益。在年度SCA风险为1.60%时,增量成本效益比(ICER)分别为95,251美元/QALY(SP)和100,797美元/QALY(HP)。在年度SCA风险为3.5%时,从SP和HP角度来看,SMART都具有很高的成本效益[ICER:53,925美元/QALY(SP),59,672美元/QALY(HP)]。在微观模拟中,SMART在各风险分层中预防了1,762例死亡(各组死亡相对风险降低1.59%)。从人群角度来看,SMART在美国45岁及以上人群中至少可预防109,839例SCA死亡。
一种用于SCA预防的SMART方法可预防死亡,并且在SCA风险较高的患者中具有成本效益。配备CPR提示的智能手机大小的袖珍AED的可用性有可能极大地改善人群健康和经济结果。