Hepatology and Liver Transplantation Unit, Department of Specialized Medicine, Udine University Hospital, Udine, Italy.
Clinical Pathology, Udine University Hospital, Udine, Italy.
J Hepatol. 2022 Jul;77(1):152-162. doi: 10.1016/j.jhep.2022.02.015. Epub 2022 Mar 10.
BACKGROUND & AIMS: The long-term immunogenicity of anti-SARS-CoV-2 vaccines in liver transplant (LT) recipients is unknown. We aimed to assess the long-term antibody response of the Pfizer-BioNTech® BNT162b2 vaccine in LT recipients compared to controls.
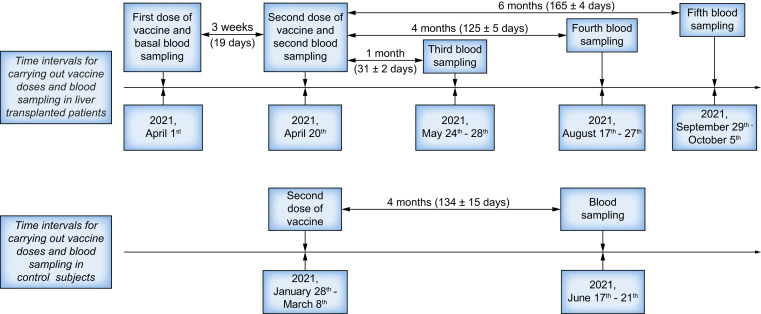
LT recipients underwent anti-SARS-CoV-2 anti-receptor-binding domain protein IgG (anti-RBD) and anti-nucleocapsid protein IgG antibody (anti-N) measurements at the first and 1, 4 and 6 months after the second vaccination dose.
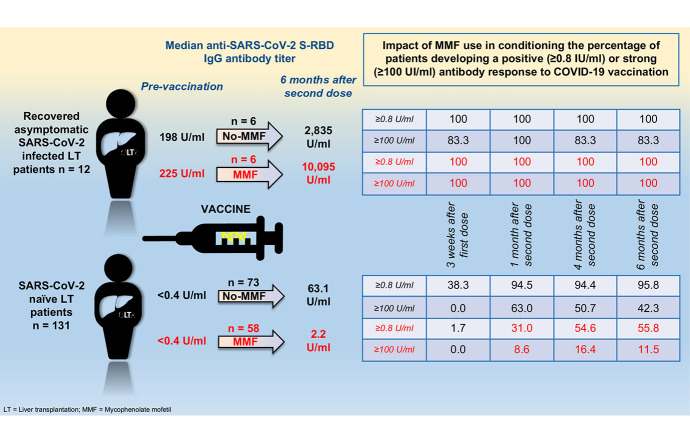
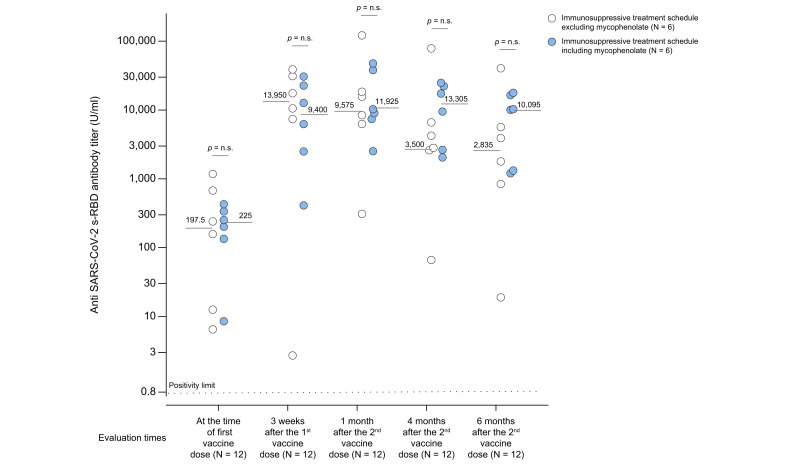
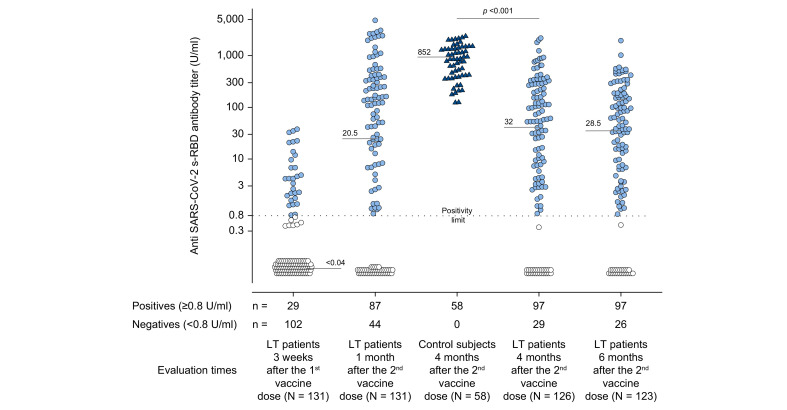
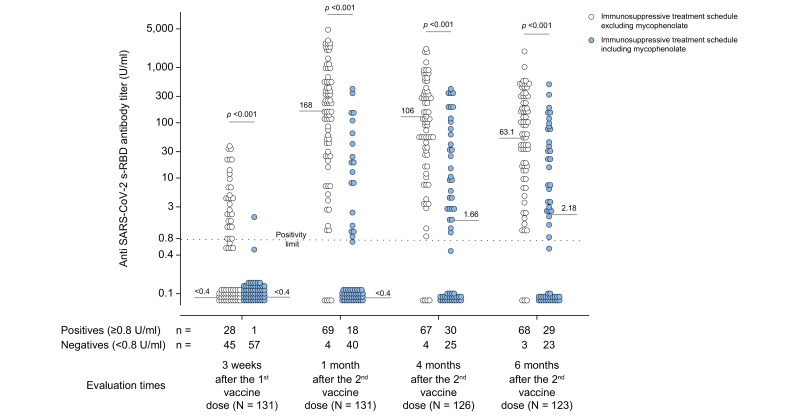
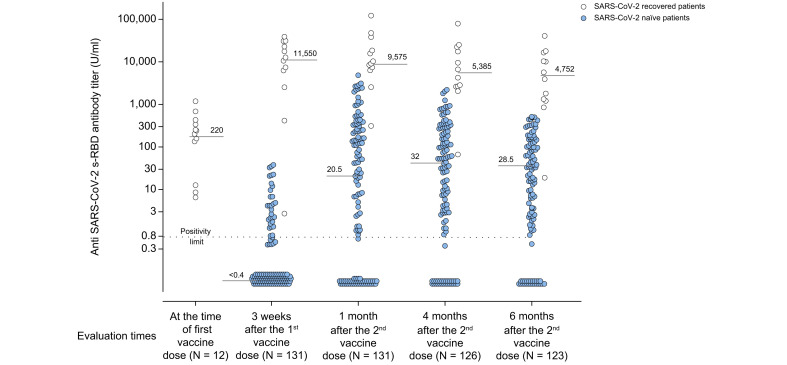
One hundred forty-three LT recipients and 58 controls were enrolled. At baseline, 131/143 (91.6%) LT recipients tested anti-N negative (COVID-19 naïve), and 12/143 (8.4%) tested positive (COVID-19 recovered) compared to negative controls. Among COVID-19 naïve, 22.1% were anti-RBD positives 1 month after the first vaccine dose, while 66.4%, 77%, and 78.8% were 1, 4 and 6 months following the second vaccine dose. In contrast, 100% of controls were positive at 4 months (p <0.001). The median anti-RBD titer 4 months after the second vaccine dose was significantly lower (32 U/ml) in COVID-19 naïve than in controls (852 U/ml, p <0.0001). A higher daily dose of mycophenolate mofetil (MMF) (p <0.001), higher frequency of ascites (p = 0.012), and lower serum leukocyte count (p = 0.016) were independent predictors of anti-RBD negativity at 6 months. All COVID-19 recovered patients tested positive for anti-RBD at each time point. The median antibody titer was similar in those taking MMF (9,400 U/ml, 11,925 U/ml, 13,305 U/ml, and 10,095 U/ml) or not taking MMF (13,950 U/ml, 9,575 U/ml, 3,500 U/ml, 2,835 U/ml, p = NS) 3 weeks after the first and 1, 4 and 6 months after the second vaccine dose, respectively.
In COVID-19-naïve LT recipients, the immunogenicity of anti-SARS-CoV-2 vaccination was significantly lower than that in controls. MMF was the main determinant of vaccination failure in SARS-CoV-2-naïve patients.
The immunogenicity of anti-SARS-CoV-2 vaccination in liver transplant recipients is currently unknown. Herein, we show that liver transplant recipients who have not previously had COVID-19 are less likely to mount effective antibody responses to vaccination than a control population. The main determinant of vaccination failure was the use of the immunosuppressive drug mycophenolate mofetil.
目前尚不清楚抗 SARS-CoV-2 疫苗在肝移植(LT)受者中的长期免疫原性。我们旨在评估与对照组相比,LT 受者在接受辉瑞-生物技术公司的 BNT162b2 疫苗后的长期抗 SARS-CoV-2 受体结合域蛋白 IgG(抗-RBD)和抗核衣壳蛋白 IgG 抗体(抗-N)应答。
LT 受者在第二次接种疫苗后第 1、1、4 和 6 个月时进行抗 SARS-CoV-2 抗受体结合域蛋白 IgG(抗-RBD)和抗核衣壳蛋白 IgG 抗体(抗-N)测量。
共纳入 143 例 LT 受者和 58 例对照。在基线时,与阴性对照组相比,131/143(91.6%)的 LT 受者抗-N 阴性(COVID-19 初治),12/143(8.4%)抗-N 阳性(COVID-19 已康复)。在 COVID-19 初治者中,第 1 次疫苗接种后 1 个月时,22.1%的患者抗-RBD 阳性,而在第 2 次疫苗接种后 1、4 和 6 个月时,分别有 66.4%、77%和 78.8%的患者抗-RBD 阳性。相比之下,对照组在 4 个月时 100%阳性(p<0.001)。第二次疫苗接种后 4 个月时,COVID-19 初治患者的抗-RBD 滴度中位数(32 U/ml)明显低于对照组(852 U/ml,p<0.0001)。更高的霉酚酸酯(MMF)日剂量(p<0.001)、更高的腹水频率(p=0.012)和更低的血清白细胞计数(p=0.016)是 6 个月时抗-RBD 阴性的独立预测因素。所有 COVID-19 已康复患者在每个时间点均检测到抗-RBD 阳性。服用 MMF 的患者(9400 U/ml、11925 U/ml、13305 U/ml 和 10095 U/ml)与未服用 MMF 的患者(13950 U/ml、9575 U/ml、3500 U/ml 和 2835 U/ml)的中位数抗体滴度相似,分别为第 1 次和第 2 次疫苗接种后 3 周、1、4 和 6 个月。
在 COVID-19 初治的 LT 受者中,抗 SARS-CoV-2 疫苗的免疫原性明显低于对照组。MMF 是 SARS-CoV-2 初治患者疫苗接种失败的主要决定因素。
目前尚不清楚肝移植受者抗 SARS-CoV-2 疫苗的免疫原性。本研究表明,与对照组相比,既往未感染过 COVID-19 的肝移植受者对疫苗接种产生有效抗体应答的可能性较低。疫苗接种失败的主要决定因素是使用免疫抑制剂霉酚酸酯。