Division of Nephrology, ICMR Center for Advanced Research in Nephrology, Department of Pediatrics, All India Institute of Medical Sciences, New Delhi, 110029, India.
Pediatr Nephrol. 2022 Dec;37(12):3117-3126. doi: 10.1007/s00467-022-05475-8. Epub 2022 Mar 14.
Rituximab and tacrolimus are therapies reserved for patients with frequently relapsing or steroid-dependent nephrotic syndrome who have failed conventional steroid-sparing agents. Given their toxicities, demonstrating non-inferiority of rituximab to tacrolimus may enable choice between these medications.
This investigator-initiated, single-center, open-label, pilot randomized controlled trial examined the non-inferiority of two doses of intravenous (IV) rituximab given one-week apart to oral therapy with tacrolimus (1:1 allocation), in maintaining sustained remission over 12 months follow-up, in patients with difficult-to-treat steroid-sensitive nephrotic syndrome, defined as frequently relapsing or steroid-dependent disease that had failed ≥ 2 steroid-sparing strategies. Secondary outcomes included frequency of relapses, proportion with frequent relapses, time to relapse and frequent relapses, and adverse events (CTRI/2018/11/016342).
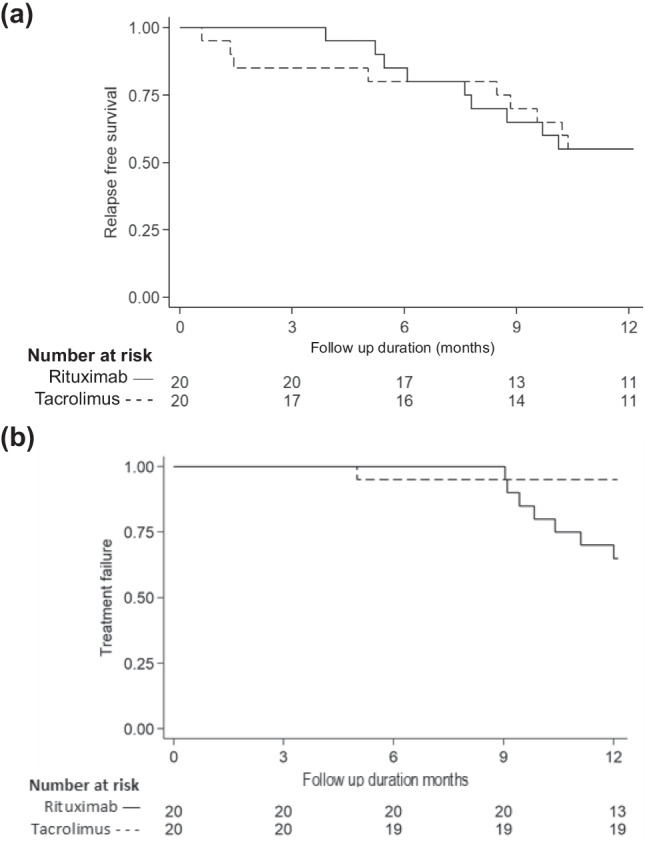
Baseline characteristics were comparable for 41 patients randomized to receive rituximab (n = 21) or tacrolimus (n = 20). While 55% of patients in each limb were in sustained remission at 1 year, non-inferiority of rituximab to tacrolimus was not demonstrated (mean difference 0%; 95% CI - 30.8%, 30.8%; non-inferiority limit - 20%; P = 0.50). Frequent relapses were more common in patients administered rituximab compared to tacrolimus (risk difference 30%, 95% CI 7.0, 53.0, P = 0.023). Both groups showed similar reductions in relapse rates and prednisolone use. Common adverse events were infusion-related with rituximab and gastrointestinal symptoms with tacrolimus.
Therapy with rituximab was not shown to be non-inferior to 12-months treatment with tacrolimus in maintaining remission in patients with difficult-to-treat steroid-sensitive nephrotic syndrome. Frequent relapses were more common with rituximab. While effective, both agents require close monitoring for adverse events. A higher resolution version of the Graphical abstract is available as Supplementary information.
利妥昔单抗和他克莫司是用于经常复发或对类固醇依赖的肾病综合征患者的治疗方法,这些患者对常规类固醇保留剂治疗无效。鉴于它们的毒性,证明利妥昔单抗不比他克莫司差,可能会使这些药物的选择成为可能。
这是一项由研究者发起的、单中心的、开放性标签的、试验性随机对照研究,检查了每间隔一周静脉注射(IV)给予两次利妥昔单抗与口服他克莫司治疗(1:1 分配),在 12 个月的随访中维持持续缓解的非劣效性,在治疗难治性类固醇敏感肾病综合征患者中,定义为经常复发或对类固醇依赖的疾病,这些疾病对≥2 种类固醇保留策略治疗失败。次要结局包括复发频率、频繁复发的比例、复发时间和频繁复发以及不良事件(CTRI/2018/11/016342)。
41 名随机接受利妥昔单抗(n=21)或他克莫司(n=20)治疗的患者的基线特征相似。虽然每个治疗组的 55%患者在 1 年内处于持续缓解状态,但利妥昔单抗不比他克莫司差(平均差异 0%;95%CI-30.8%,30.8%;非劣效性下限-20%;P=0.50)。与他克莫司相比,接受利妥昔单抗治疗的患者更常出现频繁复发(风险差异 30%,95%CI7.0,53.0,P=0.023)。两组的复发率和泼尼松使用率均相似降低。常见的不良事件与利妥昔单抗相关的输注反应和与他克莫司相关的胃肠道症状。
在维持治疗难治性类固醇敏感肾病综合征患者缓解方面,利妥昔单抗治疗 12 个月并不优于他克莫司治疗。利妥昔单抗治疗的患者更常出现频繁复发。虽然有效,但两种药物都需要密切监测不良反应。更高分辨率的图表摘要可在补充信息中获得。