Department II of Internal Medicine and Center for Molecular Medicine Cologne, Faculty of Medicine, University Hospital of Cologne, University of Cologne, Cologne, Germany.
Faculty of Medicine, Pediatric Nephrology, Children's and Adolescents' Hospital, University Hospital of Cologne, University of Cologne, Cologne, Germany.
Sci Rep. 2023 Apr 28;13(1):6980. doi: 10.1038/s41598-023-32576-7.
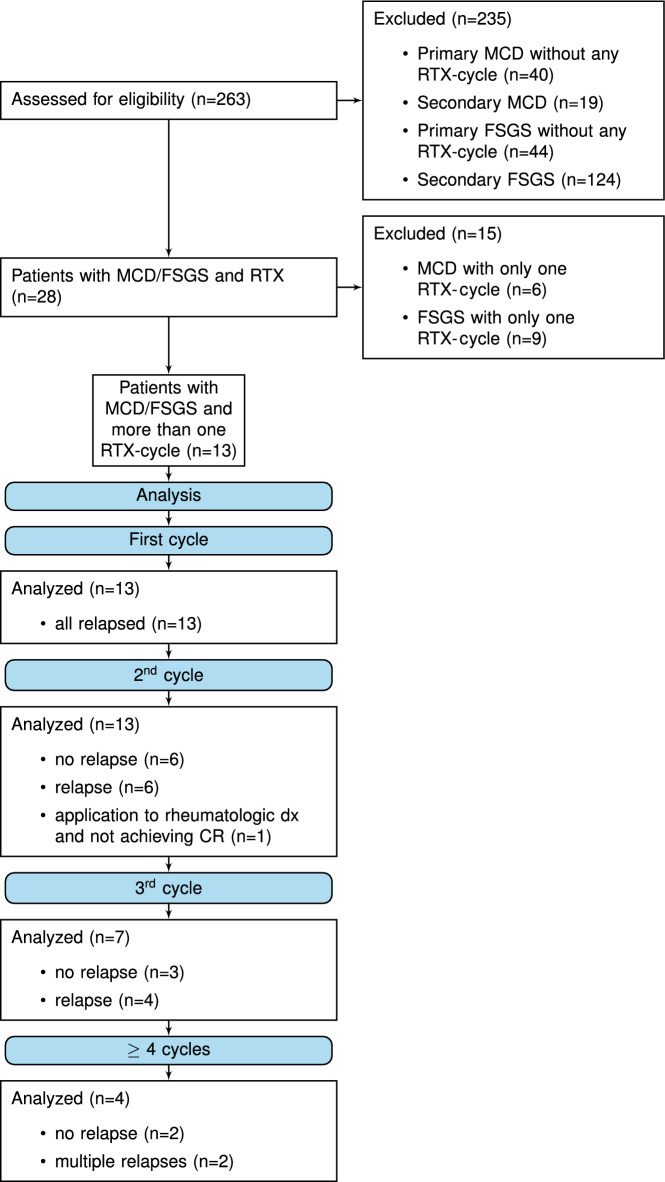
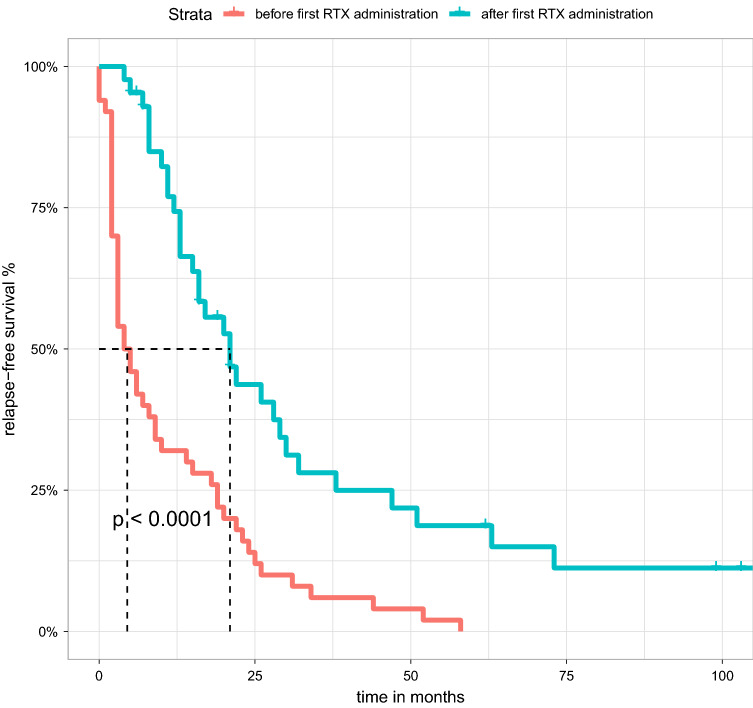
Minimal change disease (MCD) and focal segmental glomerulosclerosis (FSGS) are glomerulopathies associated with nephrotic syndrome. Primary forms of these diseases are treated with various regimes of immunosuppression. Frequently relapsing or glucocorticoid-dependent courses remain challenging. Here, a B-cell-depleting strategy with rituximab represents a salvage option although data are sparse in the adult population. In particular, there is limited evidence on the efficacy of restoring remission after initial successful treatment with rituximab and whether patients benefit from an individualized, relapse-based approach. We identified 13 patients who received multiple therapies with rituximab from the FOrMe-registry (NCT03949972), a nationwide registry for MCD and FSGS in Germany, or from the University Hospital of Cologne. Disease status, changes in serum creatinine, proteinuria, and time to relapse were evaluated. Relapse-free survival was compared to the patients' previous therapy regimens. Through all treatment cycles, an improvement of disease activity was shown leading to a complete remission in 72% and partial remission in 26% after 3 ([Formula: see text]0.001) and 6 months ([Formula: see text]0.001). Relapse-free survival increased from 4.5 months (95%-CI 3-10 months) to 21 months (95%-CI 16-32 months) ([Formula: see text]0.001) compared to previous immunosuppression regimens with no loss in estimated glomerular filtration over time (p = 0.53). Compared to continuous B-cell depletion, an individualized relapse-based approach led to a reduced rituximab exposure and significant cost savings. Relapse-based administration of rituximab in patients with MCD/FSGS with an initial good clinical response did not result in a decreased efficacy at a median follow-up duration of 110 months. Thus, reinduction therapies may provide an alternative to continuous B-cell-depletion and reduce the long-term side effects of continuous immunosuppression.
微小病变病(MCD)和局灶节段性肾小球硬化症(FSGS)是与肾病综合征相关的肾小球疾病。这些疾病的原发性形式采用各种免疫抑制方案进行治疗。频繁复发或依赖糖皮质激素的病程仍然具有挑战性。在这里,使用利妥昔单抗的 B 细胞耗竭策略代表了一种挽救选择,尽管在成人人群中数据稀缺。特别是,在最初使用利妥昔单抗成功治疗后恢复缓解的疗效以及患者是否受益于基于个体化、复发的方法方面,证据有限。我们从德国的 MCD 和 FSGS 全国登记处 FOrMe-Registry(NCT03949972)或科隆大学医院确定了 13 名接受利妥昔单抗多次治疗的患者。评估了疾病状态、血清肌酐、蛋白尿的变化以及复发时间。将无复发生存率与患者的先前治疗方案进行比较。通过所有治疗周期,显示疾病活动度改善,导致 72%的患者完全缓解和 26%的部分缓解,在 3 个月([Formula: see text]0.001)和 6 个月([Formula: see text]0.001)时。与先前的免疫抑制方案相比,无复发生存率从 4.5 个月(95%CI 3-10 个月)增加到 21 个月(95%CI 16-32 个月)([Formula: see text]0.001),而估计肾小球滤过率随时间没有丢失(p = 0.53)。与连续 B 细胞耗竭相比,基于个体化复发的方法导致利妥昔单抗暴露减少和显著的成本节约。在最初临床反应良好的 MCD/FSGS 患者中,基于复发的利妥昔单抗给药不会在中位数为 110 个月的随访期间降低疗效。因此,再诱导治疗可能是连续 B 细胞耗竭的替代方法,并减少长期的免疫抑制副作用。