Fiorito Ivan, Gori Giulia, Perrone Tiziano, Mascolo Amelia, Caimmi Silvia, Palumbo Ilaria, De Silvestri Annalisa, Delliponti Mariangela, Di Sabatino Antonio, Marseglia Gian Luigi
Department of Pediatrics, Foundation IRCCS Policlinico San Matteo, University of Pavia, Pavia, Italy.
Department of Internal Medicine, Foundation IRCCS Policlinico San Matteo, University of Pavia, Pavia, Italy.
Front Pediatr. 2022 Feb 28;10:813874. doi: 10.3389/fped.2022.813874. eCollection 2022.
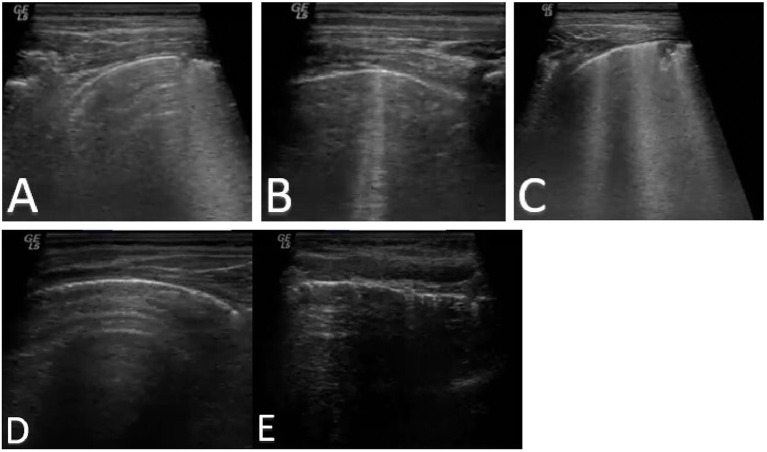
In recent years, lung ultrasound (LUS) has spread to emergency departments and clinical practise gaining great support, especially in time of pandemic, but only a few studies have been done on children. The aim of the present study is to compare the diagnostic accuracy of LUS (using Soldati LUS score) and that of chest X-ray (CXR) in CAP and COVID-19 pneumonia in paediatric patients. Secondary objective of the study is to examine the association between LUS score and disease severity. Finally, we describe the local epidemiology of paediatric CAP during the study period in the era of COVID-19 by comparing it with the previous 2 years.
This is an observational retrospective single-centre study carried out on patients aged 18 or younger and over the month of age admitted to the Paediatric Unit of our Foundation for suspected community-acquired pneumonia or SARS-CoV-2 pneumonia during the third pandemic wave of COVID-19. Quantitative variables were elaborated with Shapiro-Wilks test or median and interquartile range (IQR). Student's -test was used for independent data. Association between quantitative data was evaluated with Pearson correlation. ROC curve analysis was used to calculate best cut-off of LUS score in paediatric patients. Area under the ROC curve (AUC), sensibility, and specificity are also reported with 95% confidence interval (CI).
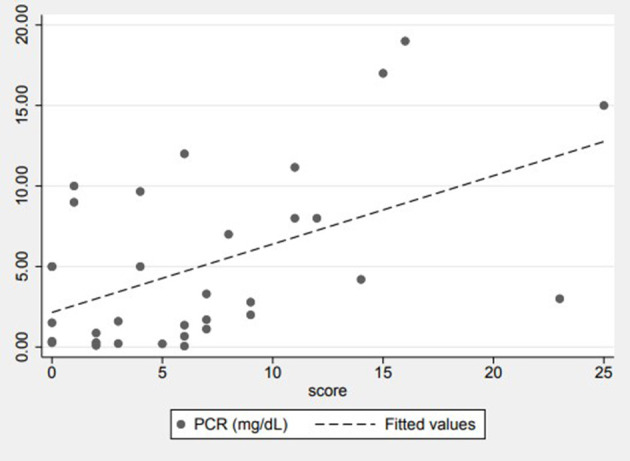
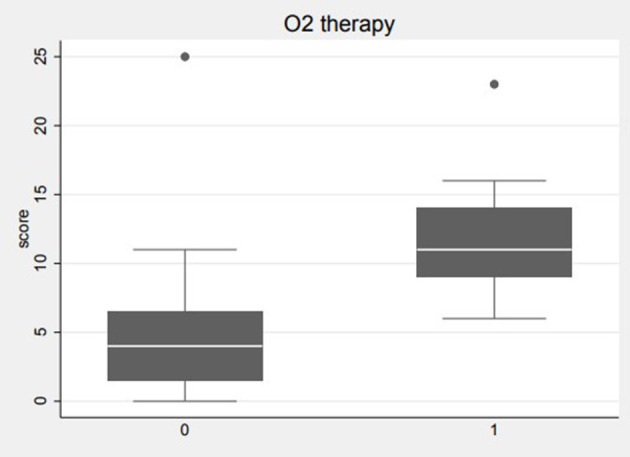
The diagnostic accuracy of the LUS score in pneumonia, the area underlying the ROC curve (AUC) was 0.67 (95% CI: 0.27-1) thus showing a discrete discriminatory power, with a sensitivity of 89.66% and specificity 50% setting a LUS score greater than or equal to 1 as the best cut-off. Nine patients required oxygen support and a significant statistical correlation ( = 0.0033) emerged between LUS score and oxygen therapy. The mean LUS score in patients requiring oxygen therapy was 12. RCP was positively correlated to the patient's LUS score ( = 0.0024).
Our study has shown that LUS is a valid alternative to CXR. Our results show how LUS score can be applied effectively for the diagnosis and stratification of paediatric pneumonia.
近年来,肺部超声(LUS)已在急诊科和临床实践中得到广泛应用并获得了大力支持,尤其是在疫情期间,但针对儿童的相关研究较少。本研究旨在比较LUS(使用索尔达蒂LUS评分)和胸部X线(CXR)对儿科患者社区获得性肺炎(CAP)和新冠肺炎肺炎的诊断准确性。该研究的次要目标是检查LUS评分与疾病严重程度之间的关联。最后,我们通过将研究期间新冠疫情时代儿科CAP的当地流行病学与前两年进行比较来进行描述。
这是一项在我们基金会儿科病房对18岁及以下且年龄超过1个月的疑似社区获得性肺炎或新冠病毒2型肺炎患者进行的回顾性单中心观察研究,该研究在新冠疫情的第三波大流行期间开展。定量变量采用夏皮罗-威尔克检验或中位数和四分位间距(IQR)进行分析。独立数据采用学生t检验。定量数据之间的关联采用皮尔逊相关进行评估。采用ROC曲线分析来计算儿科患者LUS评分的最佳截断值。同时报告ROC曲线下面积(AUC)、敏感性和特异性以及95%置信区间(CI)。
LUS评分在肺炎诊断中的准确性方面,ROC曲线下面积(AUC)为0.67(95%CI:0.27 - 1),显示出一定的鉴别能力,将LUS评分大于或等于1设定为最佳截断值时,敏感性为89.66%,特异性为50%。9名患者需要氧气支持,LUS评分与氧疗之间存在显著的统计学相关性(P = 0.0033)。需要氧疗的患者的平均LUS评分为12。呼吸频率(RCP)与患者的LUS评分呈正相关(P = 0.0024)。
我们的研究表明,LUS是CXR的有效替代方法。我们的结果表明LUS评分如何能够有效地应用于儿科肺炎的诊断和分层。