Department of Emergency Medicine, COVID Care Unit, Santa Maria Delle Grazie Hospital, Via Domitiana, 5, 80078, Pozzuoli, Naples, Italy.
Department of Translational Medical Sciences, Federico II University, Naples, Italy.
Intern Emerg Med. 2021 Mar;16(2):471-476. doi: 10.1007/s11739-020-02512-y. Epub 2020 Oct 3.
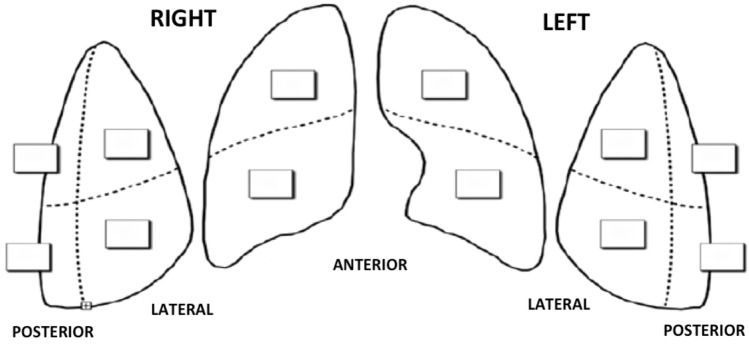
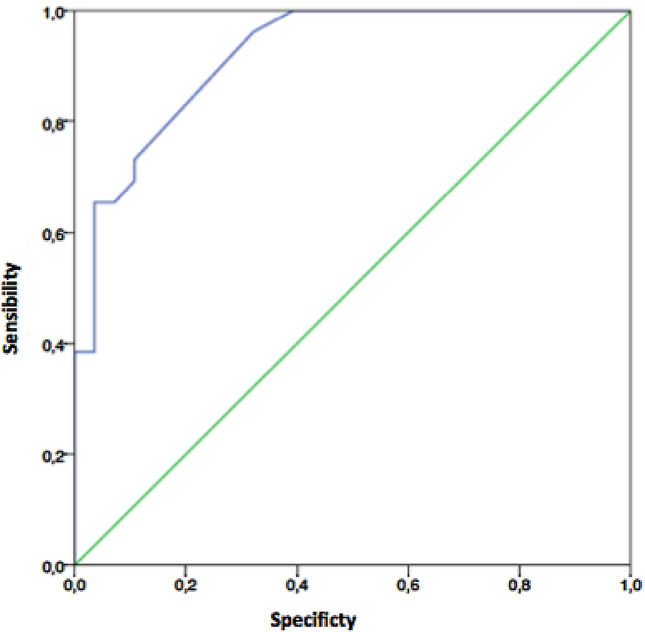
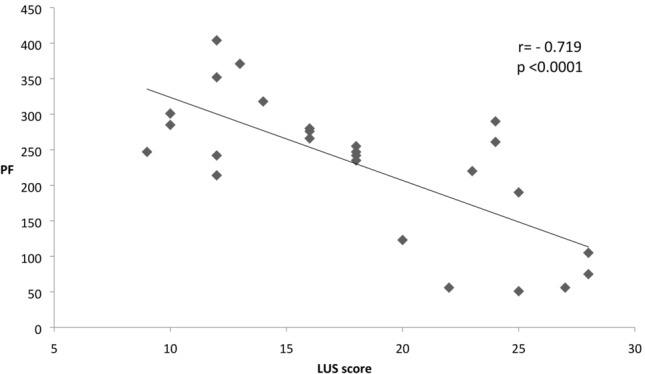
The aim of this study was to explore the role of lung ultrasound (LUS) in the diagnosis of SARS-CoV-2 infection and to verify its utility in the prediction of lung disease's severity and outcome. Fifty-three consecutive patients presenting to the Emergency Department of Santa Maria delle Grazie Hospital with high suspicion of SARS-CoV-2 infection underwent diagnostic test for SARS-CoV-2 on samples obtained from nasopharyngeal swab as well as complete proper diagnostic work-up that included clinical evaluation, laboratory tests, blood gas analyses, chest CT and LUS. A semiquantitative analysis of B-lines distribution was performed to calculate the LUS score. Patients were divided into two groups according to the results of both SARS-CoV-2 diagnostic test and other exams (Group A = pneumonia due to SARS-CoV2 infection vs Group B = no SARS-CoV2 infection and another definite diagnosis). LUS showed an excellent accuracy in predicting the diagnosis of SARS-CoV-2 infection (area under the ROC curve of 0.92 with a sensibility of 73% and a specificity of 89% a the cut-off of 12.5). LUS score was more impaired in SARS-CoV-2 patients (18.1 ± 6.0 vs 7.6 ± 5.9, p < 0.00001) and it is significantly negatively correlated with PF ratio values (r = - 0.719, p < 0.0001). An intrahospital mortality rate of 46% was found; patients with adverse outcome had significant higher value of LUS, PF, LDH, and APACHE II score. None of these parameters was predictive of mortality. LUS is a useful tool for the early detection of SARS-CoV-2 infection and for the evaluation of the disease severity, but does not predict mortality. Further studies with repeated evaluations of LUS score are needed to further explore the role of LUS in the assessment of severity in SARS-CoV-2 disease and in the monitoring of the response to treatments.
本研究旨在探讨肺部超声(LUS)在 SARS-CoV-2 感染诊断中的作用,并验证其在预测肺部疾病严重程度和结局方面的效用。53 例连续就诊于圣玛丽亚德拉格拉齐亚医院急诊科,高度怀疑 SARS-CoV-2 感染的患者,对鼻咽拭子样本进行 SARS-CoV-2 诊断检测,并进行完整的适当诊断检查,包括临床评估、实验室检查、血气分析、胸部 CT 和 LUS。对 B 线分布进行半定量分析,以计算 LUS 评分。根据 SARS-CoV-2 诊断检测和其他检查的结果,将患者分为两组(A 组=SARS-CoV-2 感染引起的肺炎与 B 组=无 SARS-CoV-2 感染和其他明确诊断)。LUS 在预测 SARS-CoV-2 感染的诊断方面具有出色的准确性(ROC 曲线下面积为 0.92,敏感度为 73%,特异性为 89%,截断值为 12.5)。SARS-CoV-2 患者的 LUS 评分更差(18.1±6.0 与 7.6±5.9,p<0.00001),与 PF 比值呈显著负相关(r=-0.719,p<0.0001)。院内死亡率为 46%;不良结局患者的 LUS、PF、LDH 和 APACHE II 评分显著较高。这些参数均不能预测死亡率。LUS 是早期发现 SARS-CoV-2 感染和评估疾病严重程度的有用工具,但不能预测死亡率。需要进一步研究重复评估 LUS 评分,以进一步探讨 LUS 在评估 SARS-CoV-2 疾病严重程度和监测治疗反应中的作用。