First Department of Internal Medicine, Kansai Medical University, Hirakata, Osaka, Japan.
Leukemia/Bone Marrow Transplant Program of BC, Division of Hematology, University of British Columbia, Vancouver, British Columbia, Canada.
Eur J Haematol. 2022 Jul;109(1):58-68. doi: 10.1111/ejh.13769. Epub 2022 Apr 13.
This retrospective chart review examined real-world healthcare resource utilization (HRU) in patients with AML ineligible for intensive therapy who received first-line systemic therapy or best supportive care (BSC).
Data were collected anonymously on patients with AML who initiated first-line hypomethylating agents (HMA), low-dose cytarabine (LDAC), other systemic therapy, or BSC. HRU endpoints included hospitalizations, outpatient consultations, transfusions, and supportive care.
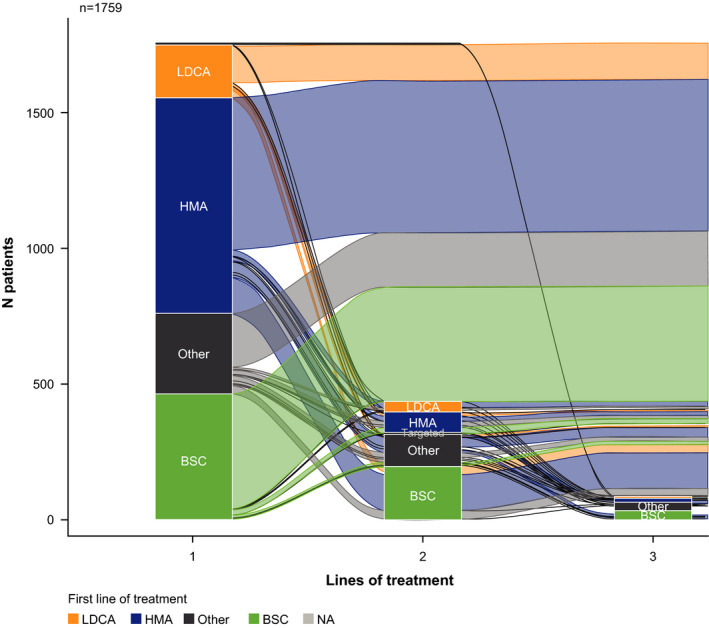
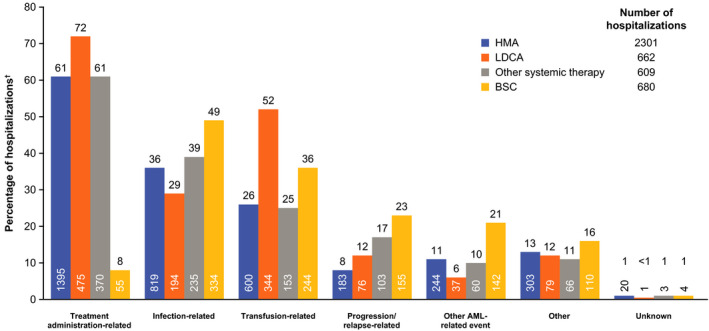
Of 1762 patients included, 46% received HMA, 11% received LDAC, 17% received other systemic therapy, 26% received BSC; median treatment durations were 118, 35, 33, and 57 days, respectively. Most patients were hospitalized, most commonly for treatment administration, transfusion, or infection (HMA 82%, LDAC 93%, other systemic therapy 83%, BSC 83%). A median number of hospitalizations were 2-6 across systemic groups and two for BSC, with median durations of 8-18 days. Transfusion rates and outpatient consultations were highest for HMA (80% and 79%) versus LDAC (57% and 53%), other systemic therapy (57% and 63%), and BSC (71% and 66%). Antivirals/antibiotics and antifungals were used more frequently than growth factors (72-92%, 34-63%, and 7-27%, respectively).
Patients with AML ineligible for intensive therapy have high HRU; novel therapies are needed to alleviate this burden.
本回顾性图表研究调查了不适合强化治疗的 AML 患者接受一线系统治疗或最佳支持治疗(BSC)的真实世界医疗资源利用(HRU)情况。
匿名收集了接受一线低甲基化剂(HMA)、低剂量阿糖胞苷(LDAC)、其他系统治疗或 BSC 的 AML 患者的资料。HRU 终点包括住院、门诊咨询、输血和支持性护理。
在纳入的 1762 名患者中,46%接受 HMA,11%接受 LDAC,17%接受其他系统治疗,26%接受 BSC;中位治疗持续时间分别为 118、35、33 和 57 天。大多数患者住院,最常见的是治疗管理、输血或感染(HMA 82%、LDAC 93%、其他系统治疗 83%、BSC 83%)。大多数系统治疗组的中位住院次数为 2-6 次,BSC 组为 2 次,中位住院时间为 8-18 天。HMA 的输血率和门诊咨询率最高(80%和 79%),其次是 LDAC(57%和 53%)、其他系统治疗(57%和 63%)和 BSC(71%和 66%)。抗病毒/抗生素和抗真菌药物的使用率高于生长因子(72%-92%、34%-63%和 7%-27%)。
不适合强化治疗的 AML 患者 HRU 较高,需要新的疗法来减轻这一负担。