Roehrkasse Amanda M, Peterson Jo Elle G, Fung Kar-Ming, Pelargos Panayiotis E, Dunn Ian F
Dunn Laboratory, Department of Neurosurgery, University of Oklahoma Health Sciences Center, Oklahoma City, OK, United States.
Department of Pathology, University of Oklahoma Health Sciences Center, Oklahoma City, OK, United States.
Front Oncol. 2022 Mar 1;12:846232. doi: 10.3389/fonc.2022.846232. eCollection 2022.
Meningiomas are the most common primary central nervous system (CNS) tumor. They are most often benign, but a subset of these can behave aggressively. Current World Health Organization (WHO) guidelines classify meningiomas into three grades based on the histologic findings and presence or absence of brain invasion. These grades are intended to guide treatment, but meningiomas can behave inconsistently with regard to their assigned histopathological grade, influencing patient expectations and management. Advanced molecular profiling of meningiomas has led to the proposal of alternative molecular grading schemes that have shown superior predictive power. These include methylation patterns, copy number alterations, and mutually exclusive driver mutations affecting oncogenes, including , and the promoter, which are associated with particularly aggressive tumor biology. Despite the evident clinical value, advanced molecular profiling methods are not widely incorporated in routine clinical practice for meningiomas.
To assess the degree of concordance between the molecular profile of meningiomas and the histopathologic WHO classification, the current method of predicting meningioma behavior.
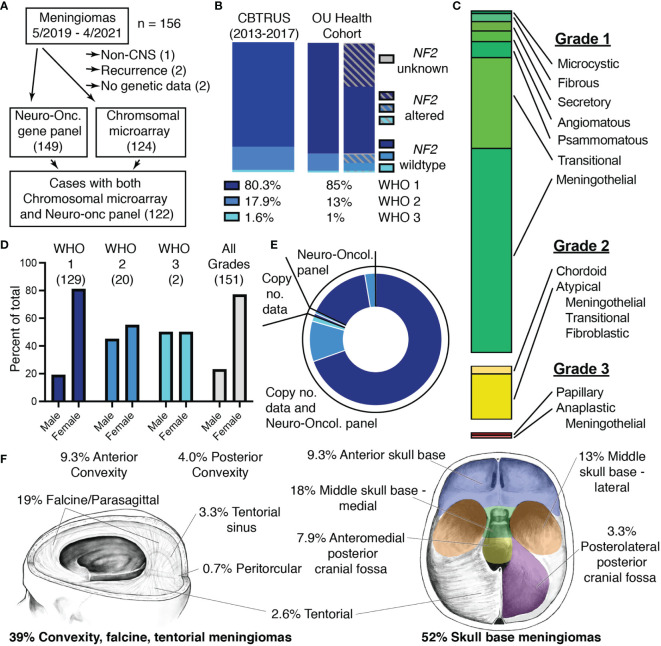
In a two-year single-institution experience, we used commercially available resources to determine molecular profiles of all resected meningiomas. Copy number aberrations and oncogenic driver mutations were identified and compared with the histopathologic grade.
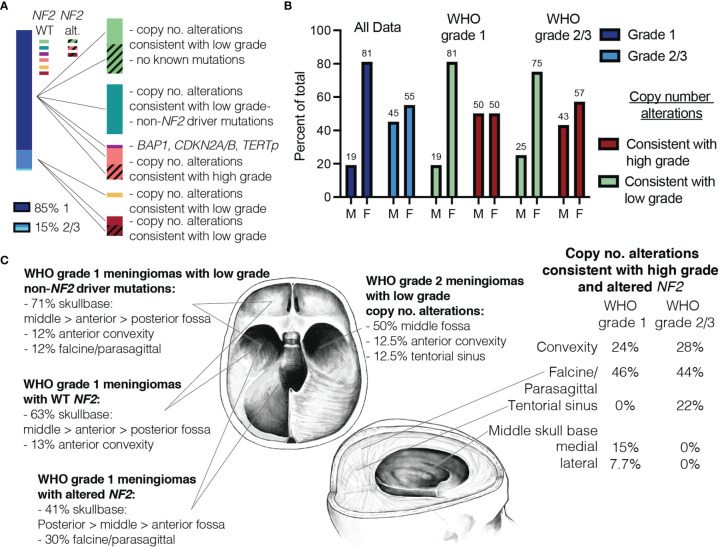
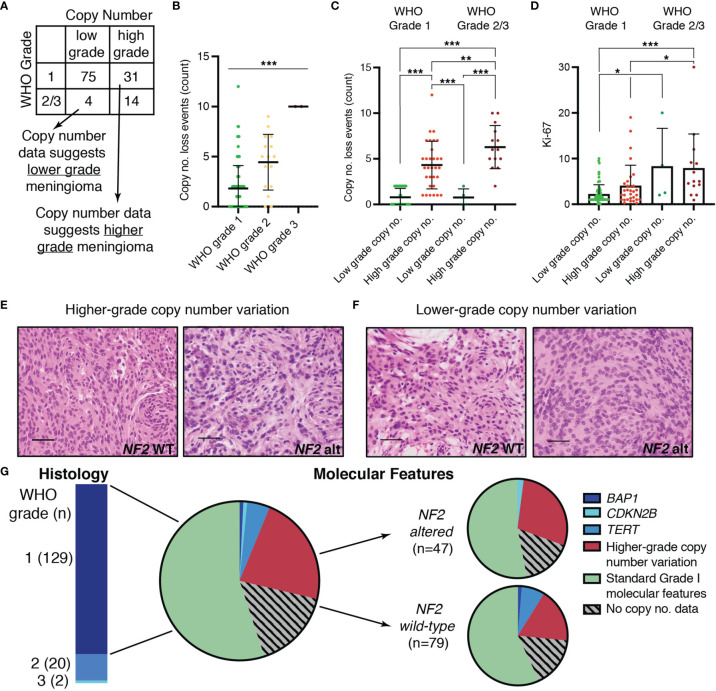
One hundred fifty-one total meningioma cases were included for analysis (85.4% WHO grade 1, 13.3% WHO grade 2, and 1.3% grade 3). Chromosomal analysis of 124 of these samples showed that 29% of WHO grade 1 tumor featured copy number profiles consistent with higher grade meningioma, and 25% of WHO grade 2 meningiomas had copy number profiles consistent with less aggressive tumors. Furthermore, 8% harbored mutations in , or of which 6% occurred in grade 1 meningiomas.
Routine advanced molecular profiling of all resected meningiomas using commercially available resources allowed for identification of a significant number of meningiomas whose molecular profiles were inconsistent with WHO grade. Our work shows the clinical value of integrating routine molecular profiling with histopathologic grading to guide clinical decision making.
脑膜瘤是最常见的原发性中枢神经系统(CNS)肿瘤。它们大多为良性,但其中一部分可能具有侵袭性。世界卫生组织(WHO)现行指南根据组织学表现及是否存在脑侵犯将脑膜瘤分为三级。这些分级旨在指导治疗,但脑膜瘤在其指定的组织病理学分级方面表现可能不一致,这会影响患者的期望和治疗管理。对脑膜瘤进行先进的分子分析已促使人们提出了具有更高预测能力的替代分子分级方案。这些方案包括甲基化模式、拷贝数改变以及影响癌基因的互斥驱动突变,包括 、 和 启动子,这些与特别侵袭性的肿瘤生物学相关。尽管具有明显的临床价值,但先进的分子分析方法在脑膜瘤的常规临床实践中并未广泛应用。
评估脑膜瘤的分子特征与组织病理学WHO分类(目前预测脑膜瘤行为的方法)之间的一致性程度。
在一项为期两年的单机构研究中,我们利用市售资源确定所有切除的脑膜瘤的分子特征。识别拷贝数畸变和致癌驱动突变,并与组织病理学分级进行比较。
共纳入151例脑膜瘤病例进行分析(WHO一级占85.4%,WHO二级占13.3%,三级占1.3%)。对其中124个样本进行的染色体分析表明,29%的WHO一级肿瘤具有与更高分级脑膜瘤一致的拷贝数特征,25%的WHO二级脑膜瘤具有与侵袭性较低肿瘤一致的拷贝数特征。此外,8%的肿瘤存在 、 或 的突变,其中6%发生在一级脑膜瘤中。
使用市售资源对所有切除的脑膜瘤进行常规先进分子分析,能够识别出大量分子特征与WHO分级不一致的脑膜瘤。我们的研究表明,将常规分子分析与组织病理学分级相结合以指导临床决策具有临床价值。