Department of Anaesthesiology and Pain Medicine, Inselspital, Bern University Hospital, Bern, Switzerland.
Department of Anaesthesiology and Pain Medicine, Inselspital, Bern University Hospital, Switzerland.
Anaesthesia. 2022 Jul;77(7):751-762. doi: 10.1111/anae.15704. Epub 2022 Mar 18.
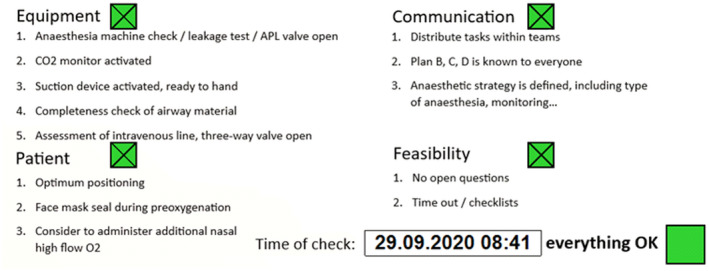
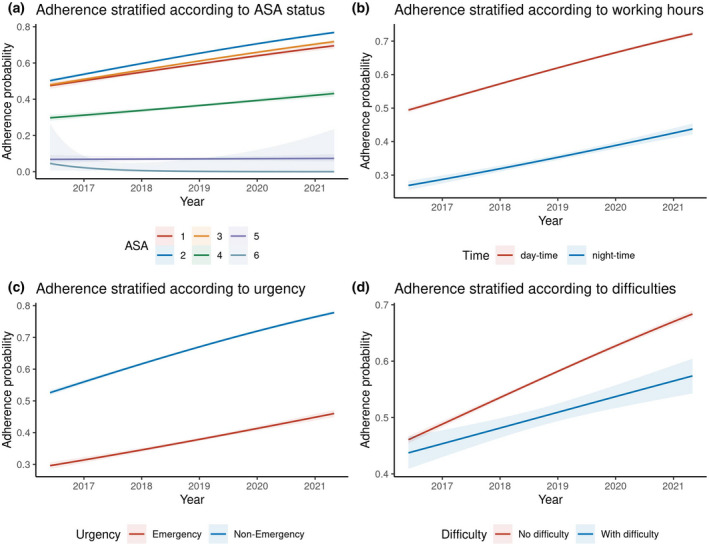
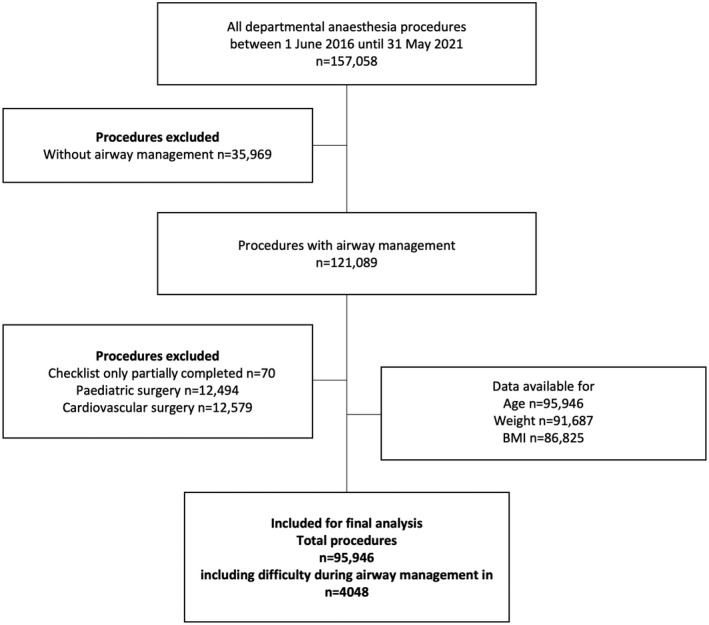
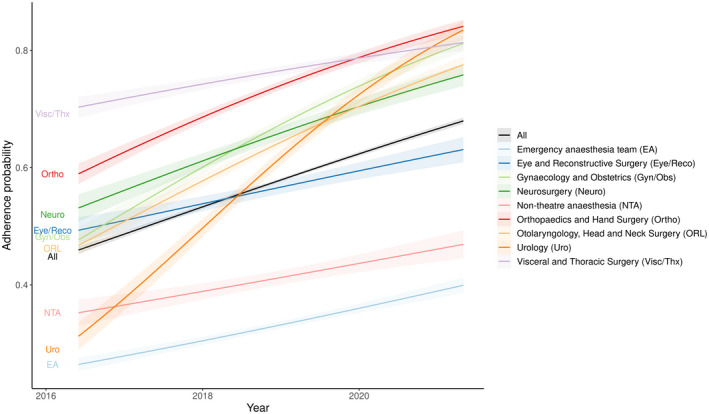
Although patient safety related to airway management has improved substantially over the last few decades, life-threatening events still occur. Technical skills, clinical expertise and human factors contribute to successful airway management. Checklists aim to improve safety by providing a structured approach to equipment, personnel and decision-making. This audit investigates adherence to our institution's airway checklist from 1 June 2016 to 31 May 2021. Inclusion criteria were procedures requiring airway management and we excluded all procedures performed solely under regional anaesthesia, sedation without airway management or paediatric and cardiovascular surgery. The primary outcome was the proportion of wholly performed pre-induction checklists. Secondary outcomes were the pattern of adherence over the 5 years well as details of airway management, including: airway management difficulties; time and location of induction; anaesthesia teams in operating theatres (including teams for different surgical specialities); non-operating theatre and emergency procedures; type of anaesthesia (general or combined); and urgency of the procedure. In total, 95,946 procedures were included. In 57.3%, anaesthesia pre-induction checklists were completed. Over the 5 years after implementation, adherence improved from 48.3% to 66.7% (p < 0.001). Anticipated and unanticipated airway management difficulties (e.g. facemask ventilation, supraglottic airway device or intubation) defined by the handling anaesthetist were encountered in 4.2% of all procedures. Completion of the checklist differed depending on the time of day (61.3% during the day vs. 35.0% during the night, p < 0.001). Completion also differed depending on location (66.8% in operating theatres vs. 41.0% for non-operating theatre anaesthesia, p < 0.001) and urgency of procedure (65.4% in non-emergencies vs. 35.4% in emergencies, p < 0.001). A mixed-effect model indicated that urgency of procedure is a strong predictor for adherence, with emergency cases having lower adherence (OR 0.58, 95%CI 0.49-0.68, p < 0.001). In conclusion, over 5 years, a significant increase in adherence to an anaesthesia pre-induction checklist was found, and areas for further improvement (e.g. emergencies, non-operating room procedures, night-time procedures) were identified.
尽管过去几十年中,与气道管理相关的患者安全已得到大幅改善,但危及生命的事件仍时有发生。技术技能、临床专业知识和人为因素有助于实现成功的气道管理。清单旨在通过提供设备、人员和决策的结构化方法来提高安全性。本次审核调查了我们机构从 2016 年 6 月 1 日至 2021 年 5 月 31 日期间的气道清单执行情况。纳入标准为需要气道管理的程序,我们排除了所有仅在区域麻醉下进行的程序、无气道管理的镇静或儿科和心血管手术。主要结局是完全执行诱导前清单的比例。次要结局是 5 年内的依从模式以及气道管理的详细信息,包括:气道管理困难;诱导的时间和地点;手术室中的麻醉团队(包括不同手术专业的团队);非手术室和紧急程序;麻醉类型(全身或联合);以及程序的紧急程度。总共有 95946 例程序被纳入。在 57.3%的情况下,完成了麻醉诱导前的清单。在实施后的 5 年内,依从性从 48.3%提高到 66.7%(p<0.001)。由处理麻醉师定义的预期和意外气道管理困难(例如面罩通气、声门上气道装置或插管)在所有程序中占 4.2%。清单的完成情况因一天中的时间而异(白天为 61.3%,晚上为 35.0%,p<0.001)。完成情况还因地点而异(手术室为 66.8%,非手术室麻醉为 41.0%,p<0.001)和程序的紧急程度而异(非紧急情况为 65.4%,紧急情况为 35.4%,p<0.001)。混合效应模型表明,程序的紧急程度是依从性的一个强有力预测因素,紧急情况的依从性较低(OR 0.58,95%CI 0.49-0.68,p<0.001)。总之,在 5 年内,发现对麻醉诱导前清单的依从性显著增加,并确定了进一步改进的领域(例如,紧急情况、非手术室程序、夜间程序)。